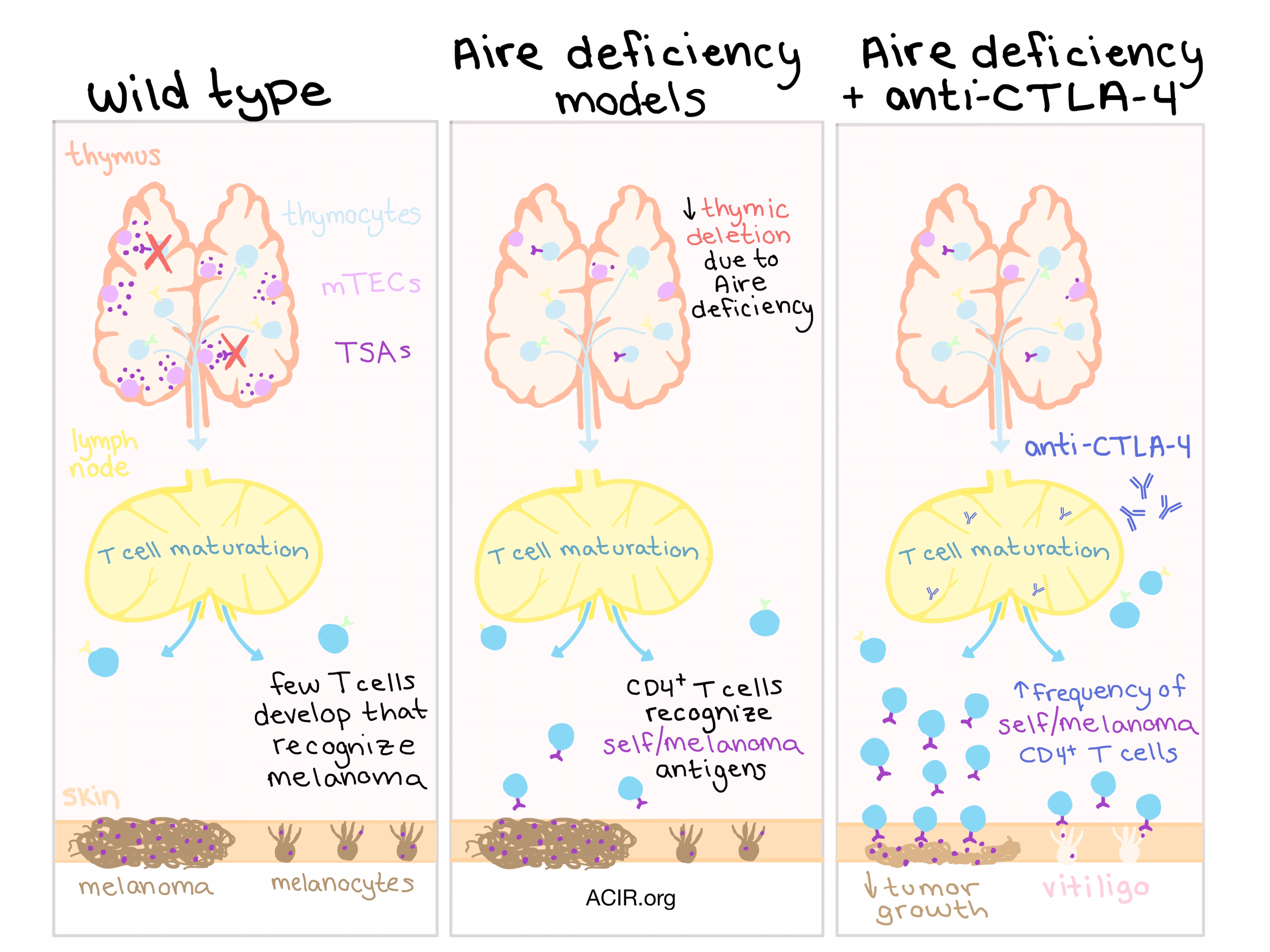
Central tolerance is essential for protection against autoimmune reactions, but cancers being so similar to “self”, this protective mechanism sometimes limits the immune system’s ability to fight off cancerous cells. Autoimmune regulator (Aire) is a regulator of central tolerance that is expressed predominantly in medullary thymic epithelial cells (mTECs) in the thymus. The expression of Aire protects against autoimmunity by promoting the expression of tissue-restricted self-antigens (TSAs) so that nearby self-reactive thymocytes with high-affinity T cell receptors (TCRs) that recognize these TSAs are deleted, losing the opportunity to develop into autoreactive T cells. Some self-antigens, however, are also highly expressed in certain cancers; MAGE-1, for example, is highly expressed in melanoma, as well as in normal melanocytes. Thus, in the context of melanoma immunotherapy, Aire-induced expression during the process of central tolerance limits the number of T cells available to react to self/melanoma antigens.
In humans, a deficiency in Aire caused by a single-nucleotide polymorphism (SNP) that is thought to reduce the stability of Aire mRNA has previously been associated with protection against melanoma and with an increase in the frequency of T cell clones recognizing MAGE-1. Bakhru et al. hypothesized that CTLA-4 checkpoint blockade might be particularly effective in animals with defective immune tolerance due to the distinct timing and mechanisms of action of these two modalities. Using a mouse model with one mutant copy of the Aire gene and thus partial loss of Aire function and increased anti-melanoma immunity (AireGW/+ mice), they observed that the addition of anti-CTLA-4 decreased B16 melanoma growth while it had no effect in wild type (WT) mice, suggesting that the combination of Aire deficiency and CTLA-4 blockade had an additive effect.
To determine which pool of cells was responsible for the observed antimelanoma efficacy, Bakhru et al. tested both CD4+ and CD8+ T cells from WT and AireGW/+ mice for reactivity against B16 melanoma. Surprisingly, they found that CD4+ T cells from Aire-deficient mice had increased cytolytic capacity against B16 melanoma cells compared to CD4+ T cells from WT mice, while no difference was observed in CD8+ T cells between the models. This suggests that antitumor immunity in the Aire-deficient context is mediated by melanoma-reactive CD4+ T cells that were rescued from thymic destruction due to Aire deficiency and were further activated by CTLA-4 in the periphery. Further, the researchers noted that CD4+ T cells from AireGW/+ mice showed increased expression of Ki67 (a marker of proliferation), increased expression of cytotoxicity-associated genes, and increased production of the cytolytic agent granzyme B. Interestingly, the frequency of granzyme B-producing CD8+ T cells was quite low among all groups, regardless of Aire deficiency or CTLA-4 blockade.
Knowing from previous studies that MAGE-1 plays a key role in Aire deficiency-mediated anti-melanoma immunity, the investigators explored whether another self/melanoma antigen - TRP-1 - played a role in the antitumor immunity. Using AireGW/+ mice treated with anti-CTLA-4, they found that T cells recognizing this antigen were preferentially expanded, and using TRP-1 TCR transgenic mice, determined that TRP-1-specific CD4+ T cells mediated additive anti-melanoma effects. Tumor growth was completely prevented in Aire-deficient mice treated with anti-CTLA-4, and mice in this group showed signs of vitiligo, a biomarker often associated with effective melanoma immunotherapy and indicating autoimmune destruction of normal melanocytes. As an evaluation of potential toxicity of this combination therapy, Bakhru et al. evaluated the severity of autoimmune colitis and confirmed that Aire deficiency did not exacerbate this known side-effect of anti-CTLA-4.
Shifting towards exploring the possible clinical potential of Aire deficiency in combination with CTLA-4 checkpoint blockade, Bakhru et al. employed an anti-RANKL antibody to block RANKL, which is critical to the survival of Aire-expressing mTECs. When the team tested a combination of anti-RANKL and anti-CTLA-4 in C57BL/6 polyclonal mice, they observed no additive effects, prompting a switch to the more effective GVAX-vaccinated C57BL/6 mouse model. They observed a significant survival benefit in GVAX-vaccinated mice co-treated with anti-RANKL and anti-CTLA-4-treated compared to GVAX-vaccinated mice treated with either antibody alone, suggesting that in the context of GVAX, anti-RANKL and anti-CTLA-4 have additive effect and improve survival in melanoma-bearing mice. An analysis of CD4+ T cells from these mice showed that anti-RANKL-induced Aire deficiency produced proliferative and cytotoxic CD4+ T cells, resembling results seen in mice with genetic Aire deficiency.
From a clinical perspective, the possibility of using anti-RANKL in combination with anti-CTLA-4 to treat melanoma is highly appealing, as both drugs are already FDA-approved. It is also possible that this therapy could extend to other cancers in which immune reactivity to tumor antigens is limited by central tolerance to TSAs. Further preclinical trials will be necessary, however, before this therapy can translate to a clinical setting.
by Lauren Hitchings



