Drugs targeting the PD-1/PD-L1 axis, like nivolumab, have revolutionized treatment of patients with metastatic melanoma. However, many patients still either do not respond or develop resistance to therapy. In an effort to modulate tumor microenvironments (TMEs) to enhance responses to anti-PD-1 therapy, Kjeldsen and Lorentzen et al. tested an immune-modulatory vaccine, IO102/IO103, to induce cytotoxic T cells against IDO and PD-L1. This strategy takes aim at both cancer cells and associated suppressive immune cells, with the goal of modulating TMEs to support responses to anti-PD-1. In a phase I/II clinical trial, MM1636, this strategy was put to the test, with the primary endpoints being safety and feasibility, and secondary endpoints being clinical efficacy and immunogenicity. The results for the first cohort of patients in this trial were recently reported in Nature Medicine.
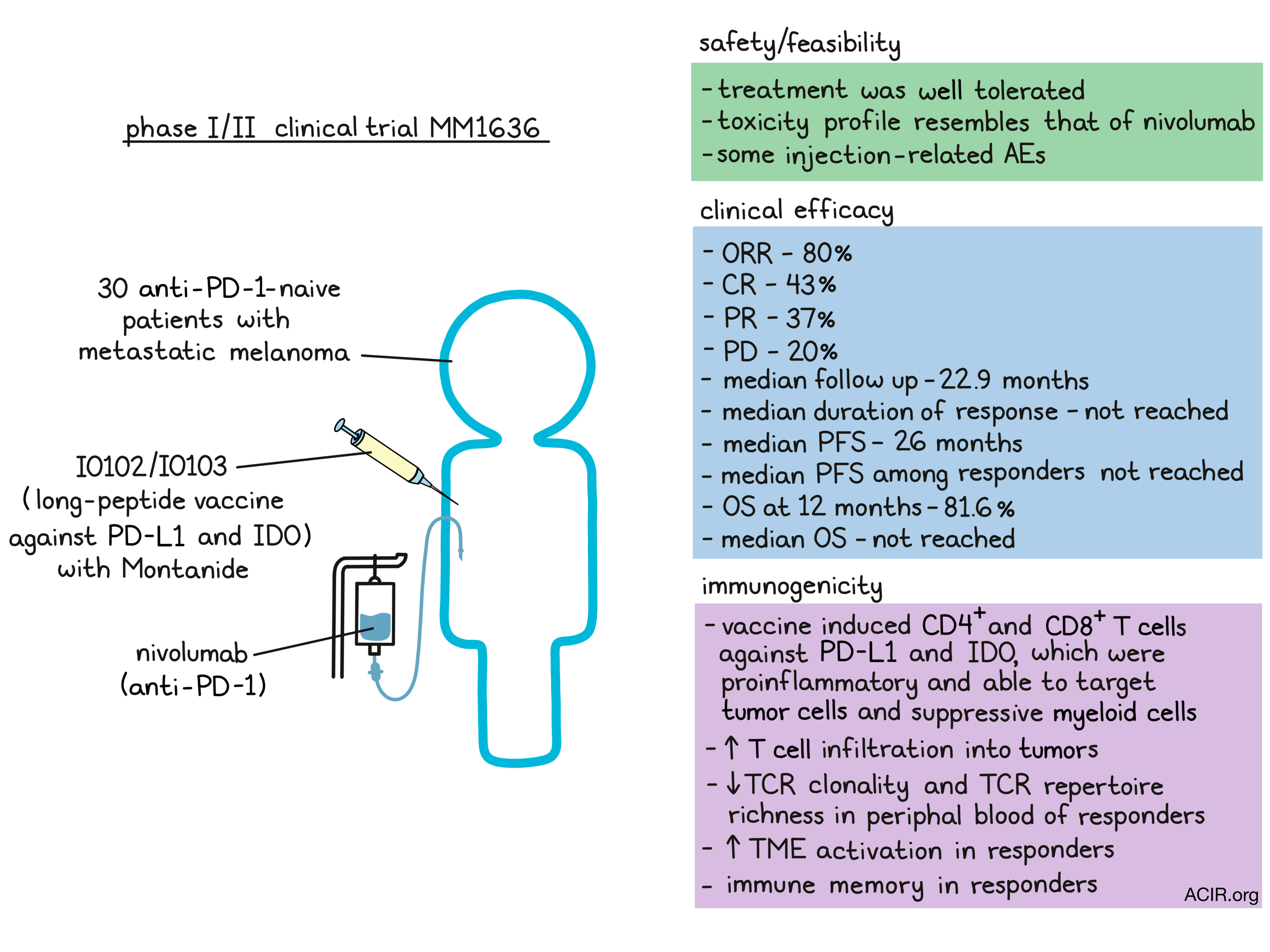
In the MM1636 trial, 30 patients with metastatic melanoma who were naive to anti-PD-1 were treated with an IDO/PD-L1 long peptide vaccine (IO102/IO103) with the adjuvant Montanide. Doses were administered every other week for the first 6 doses, then every fourth week for any additional doses. Patients received between 3 and 15 doses, with a mean of 10.5 doses. Nivolumab was given in parallel, every other week during vaccination, and every fourth week after vaccination. Several patients remained on treatment at the time of data cutoff.
Overall, the primary endpoints of the study were met, as treatment was safe and well tolerated, with a toxicity profile resembling that of nivolumab monotherapy. Grade 1-2 adverse events (AEs) were common. Four patients experienced grade 3-4 AEs, and one patient died of nivolumab-associated toxicity. AEs attributed to the vaccine were limited, with only injection site reactions being exclusive to the vaccine. Two patients decided to discontinue treatment due to granulomas, tenderness, and pain related to the injection, which were most likely due to the adjuvant Montanide.
Among the 30 treated patients, the overall responses rate (ORR) was 80%, with 43% complete responses (CRs) and 37% partial responses (PRs). The remaining 20% of patients experienced progressive disease. Responses were observed early in treatment, with 22 of 30 patients showing evidence of response at the first evaluation at 12 weeks on treatment. The median time to PR was 75 days, and the median time to CR was 327 days. The ORR among PD-L1+ patients was 94.1%, while the ORR in PD-L1- patients was 61.5%. Comparative external review determined that the ORR was 76.6%, with 53.3% CR, 23.3% PR, and 3.3% SD.
To evaluate the contribution of the IO102/IO103 vaccine, the researchers identified a matched historical control group (for 29 patients) that had been treated with nivolumab monotherapy. Compared to the controls, patients treated with the vaccine plus nivolumab had a higher ORR (79.9% vs. 41.7%), with a higher percentage of CRs (41.4% vs. 12%). The data for the response rates in the matched control group were consistent with data from larger-scale studies for patients treated with nivolumab monotherapy.
Patients were followed for up to 35 months, with a median follow-up of 22.9 months. At the time of data cutoff, a median duration of response had not been reached, with 87% of responding patients free from progression at 12 months. The median PFS for all treated patients was 26 months, and the median PFS among responders was not reached. The OS at 12 months was 81.6%, and the median OS for all patients was not reached. In the matched historical control group, the median PFS was 8.3 months and the median OS was 23.2 months.
To evaluate vaccine-induced immune responses, the researchers compared PBMC samples taken before and during therapy. Prior to treatment, 10 patients (33%) had T cell responses to IDO, 8 (27%) had responses to PD-L1, and 4 (13.3%) had responses to both. During vaccination, IDO-specific responses were detected in 28 patients (93%), and PD-L1-specific responses were detected in 26 patients (86%). Immune responses were induced in patients regardless of clinical response, suggesting that other factors contributed to clinical responsiveness. In several patients who did experience durable clinical responses, immune responses were maintained 3 and 6 months after the last vaccine, suggestive of immunological memory.
IDO- and PD-L1-specific T cells isolated from PBMC samples and expanded in vitro consisted of both CD4+ and CD8+ T cells, and showed pro-inflammatory properties, including expression of CD107a and secretion of IFNγ and TNFα. Vaccine-specific T cells were able to recognize target molecules on cancer cell lines (as long as they also expressed HLA-II) and on a peptide-pulsed myeloid cell line. Further, responses were enhanced against CD14+ myeloid cells that were induced with tumor cell-conditioned medium to express PD-L1 and IDO. Vaccine-specific responses could also be detected in PBMC samples and in the skin.
Next, the researchers used patient blood and biopsy samples to identify enriched IDO/PD-L1-specific T cell clones, and track clonal expansion upon vaccination. This revealed that IDO- and PD-L1-specific T cell clones increased in the periphery at different time points. While enrichment of vaccine-specific clones was not associated with clinical response, responders did show an increase in the T cell fraction and a decrease in TCR clonality and TCR repertoire richness, while non-responders showed the opposite. Further, highly expanded clones were frequently present before treatment and were later associated with tumors, consistent with peripherally expanded clones trafficking to tumor sites. In tumor biopsy samples, an influx of T cells after treatment was observed in responding patients.
Evaluating other treatment-induced inflammation in the TME, Kjeldsen and Lorentzen et al. found upregulated expression of genes related to adaptive immunity, such as T cell activation, effector functions, and cytotoxicity in post-treatment biopsies. They also identified increased expression of genes relating to checkpoint inhibitors (encoding TIM3, IDO, PD-L1, PD-L2, PD-1, and CTLA-4) within tumors, and upregulation of PD-L1, IDO, MHC-I and MHC-II on tumor cells in responders. Additionally, in IHC analyses of biopsies from responders, the distance between CD8+ T and PD-L1-expressing cells in biopsies was reduced compared to non-responders.
Together, these early clinical data show that the addition of the IO102/IO103 vaccine to nivolumab can induce T cell responses against PD-L1 and IDO, modulate the TME, and enhance clinical responses to anti-PD-1. While this was a small, single-center, non-randomized trial, these early results show a mPFS that is more than double that of nivolumab alone, and a notably higher ORR for PD-L1- patients. A larger randomized trial would reveal more.
Write-up and image by Lauren Hitchings
Meet the researcher
This week, Cathrine Lund Lorentzen, MD, PhD student at CCIT-DK answered our questions.

What prompted you to tackle this research question?
At the National Center for Cancer Immune Therapy (CCIT-DK), we aimed to combine an immune checkpoint inhibitor (ICI) with a type of therapy that would increase response rates and provide durable responses in patients with advanced melanoma, without inducing the amount of toxicity observed in combination ICI treatment. Previous research at CCIT-DK showed spontaneous T cell reactivity against the proteins PD-L1 and IDO in the tumor microenvironment and in the peripheral blood in both patients with cancer and healthy donors. IDO- and PD-L1-specific CD8+ T cells both recognized and killed IDO+ and/or PD-L1+ tumor cells and immunosuppressive cells.
Based on these results, we planned a clinical trial combining nivolumab with a peptide vaccine designed to engage and activate IDO- and PD-L1-specific T cells to induce a potent anti-cancer immune response in patients with metastatic melanoma, where nivolumab is used as standard of care.
What was the most surprising finding of this study for you?
The objective response rate (ORR) to nivolumab monotherapy in treatment-naive patients is around 45%. The ORR in this trial was 80%, with 43% of the patients obtaining complete responses (CR). After a median follow-up of 32 months, the median progression-free survival (PFS) was 26 months, which is twice the expected for patients receiving standard-of-care treatment. Surprisingly, the impressive response rates and survival data were also detected in the patients with unfavorable prognostic baseline characteristics at inclusion.
What was the coolest thing you’ve learned (about) recently outside of work?
I recently learned that the English Mastiff is one of the largest and heaviest dog breeds in the world. An acquaintance of mine has an English Mastiff weighing 100 kg. Despite its size, it often sits on the couch with the rest of the family. Even though I have seen pictures, I still find it hard to believe that dogs that size exist.



