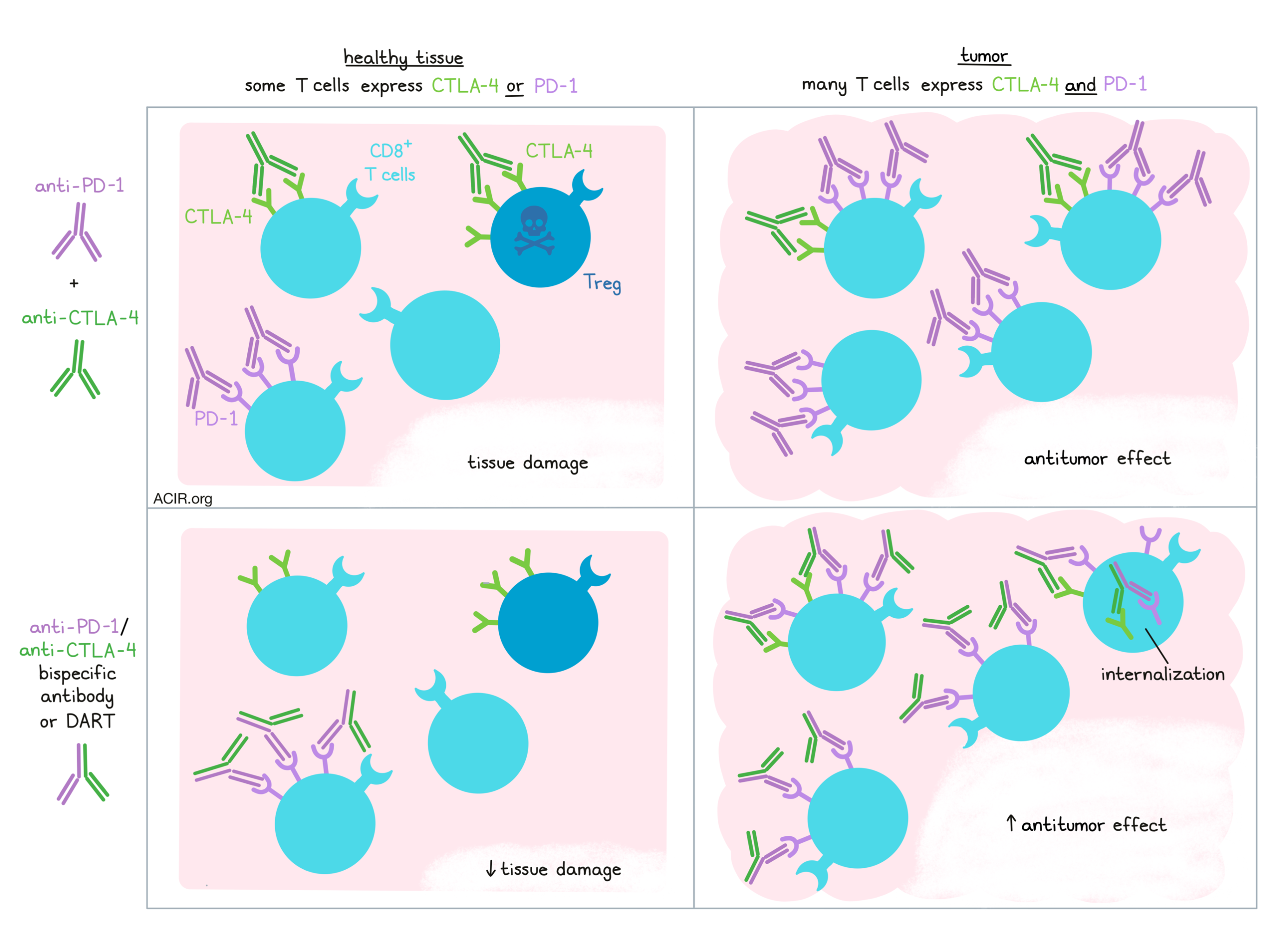
Dual blockade of PD-1 and CTLA-4 checkpoint molecules using monoclonal antibodies has taken advantage of their distinct and complementary mechanisms to enhance clinical responses over monotherapies. However, many patients still fail to respond, and over half of patients experience severe treatment-related adverse events. To improve upon these outcomes, researchers have investigated bispecific targeting strategies that can restore both immune checkpoints focused at the tumor site. In two recent reports, Berezhnoy and Sumrow et al. (in Cell Reports Medicine) and Dovedi et al. (in Cancer Discovery) engineered dual PD-1- and CTLA-4-targeting molecules to enhance target binding while limiting toxicity.
Both teams of researchers began by characterizing PD-1 and CTLA-4 expression patterns within tumors and healthy tissues. In various cancers, Berezhnoy and Sumrow et al. observed significantly higher proportions of PD-1+CTLA-4+ cells, which were mainly tumor infiltrating lymphocytes (TILs), compared to in normal tissues. These double-positive cells were also detected in the blood of cancer patients, but not healthy donors. Similarly, Dovedi et al. found PD-1- and CTLA-4-expressing CD4+ and CD8+ T cells among TILs from several cancer types, and the vast majority (80-90%) of tissue sections from multiple other cancers displayed PD-1+CTLA-4+ cell infiltration. Taken together, these results suggest that dual expression of PD-1 and CTLA-4 is a feature of the tumor microenvironment, rather than healthy tissues, opening the door for a bispecific targeting approach to potentially minimize off-target effects.
To achieve this goal, the authors engineered therapeutics capable of binding both PD-1 and CTLA-4 on the same cell (in cis). Dovedi et al. generated a bispecific PD-1 and CTLA-4 antibody (MEDI5752) using a DuetMab backbone, a technology previously developed for efficient bispecific antibody production [1], and mutated its IgG1 backbone to avoid Fc effector engagement. Berezhnoy and Sumrow et al. used the DART platform [2], recently reported for engineering antibodies with multiple independent antigen-binding sites, to construct a tetravalent (2x anti-PD-1, 2x anti-CTLA-4) molecule (MDG019). This molecule was built on an IgG4 backbone, again to reduce Fc-mediated effector functions.
Next, the researchers investigated the binding efficiencies of the bispecific constructs on target-expressing cells. Both MEDI5752 and MDG019 capably bound PD-1- and CTLA-4-expressing cell lines in cis. Interestingly, the therapeutics saturated CTLA-4 binding at much lower concentrations on PD-1+CTLA-4+ double-positive cells than on PD-1-CTLA-4+ single-positive cells, suggesting that co-engagement with PD-1 improves CTLA-4 binding. Indeed, saturating PD-1 with excess anti-PD-1 mAb before applying MDG019 or MEDI5752 reduced the efficiency of CTLA-4 binding (assessed through blocking ability and T cell IL-2 secretion, respectively). Testing in vitro efficacy in peripheral blood-derived cells, both bispecifics elicited IL-2 production better or comparable to the combination of anti-PD-1 and anti-CTLA-4 antibodies, as well as IFNγ secretion with MEDI5752. Furthermore, MDG019 did not deplete Tregs in vitro. Overall, these results were a positive sign for avoiding antibody binding to CTLA-4 in healthy tissues, in which PD-1 and CTLA-4 were less commonly co-expressed.
As the internalization kinetics of cell surface receptors play a key role in drug targeting, Dovedi et al. hypothesized that CTLA-4, which is rapidly recycled, may affect PD-1 when linked through the bispecific molecule. As anticipated, MEDI5752 and anti-CTLA-4 mAb, but not anti-PD-1 mAb quickly internalized in Chinese hamster ovary (CHO) cells or primary T cells expressing CTLA-4 and PD-1. Strikingly, MEDI5752 treatment also diminished PD-1 signal on the cell surface. Further investigation uncovered that MEDI5752, but not the combination of anti-PD-1 and anti-CTLA-4, induced colocalization of these receptors, which then colocalized with lysosomes, indicating that the linkage of CTLA-4 and PD-1 through MEDI5752 led to both of their internalizations. Concordantly, western blotting for PD-1 showed degradation after MEDI5752 treatment. These findings were confirmed in TILs derived from NSCLC, in which the bispecific therapy downregulated PD-1 more than the mAb combination. Thus, the bispecific antibodies may inhibit PD-1 signaling through receptor internalization, a mechanism only possible through dual receptor engagement, as well as a direct blockade.
Next, the researchers tested preclinical safety, efficacy, and pharmacokinetic features of their therapeutics in vivo. Dovedi et al. employed transgenic mice expressing human PD-1 and CTLA-4 and bearing MCA205 or OE21 tumors, and found that MEDI5742 was a more effective therapy than the combination of anti-PD-1 and anti-CTLA-4 antibodies. Importantly, MEDI572 accumulated within tumors more effectively than anti-CTLA-4 or isotype antibodies, but identical to anti-PD-1 antibodies, potentially limiting CTLA-4-based adverse events in the periphery. In cynomolgus monkeys, Berezhnoy and Sumrow et al. injected doses of MDG019 up to 100mg/kg, all of which were well tolerated and safe. Treatment increased the proportion of circulating memory T cells and splenic ICOS-expressing CD4+ T cells without altering Treg populations. Compared to anti-PD-1 mAb, MDG019 improved T cell proliferation (Ki67 expression).
Both reports concluded with promising early clinical results. In a dose escalation trial of 33 patients with diverse advanced solid tumors, MDG019 was tolerated up to 10mg/kg, the highest dose tested, although 80% of patients experienced adverse events (generally low grade). The therapy increased the proportion of blood Ki67+CD8+ T cells, upregulated ICOS on CD4+ T cells, and did not diminish the Treg fraction. Excitingly, four patients who had previously resisted therapy demonstrated objective responses to MDG019 treatment, including one complete response. Similarly, MEDI5752 is currently being tested in a clinical trial. Two anecdotal reports of patients with >60% tumor reduction and manageable toxicities indicate that this therapy is safe and may be effective, with upcoming data on pharmacokinetics and efficacy.
In summary, cooperative binding of both PD-1 and CTLA-4 offers a promising strategy to reverse tumor-mediated immunosuppression while avoiding healthy tissue toxicity. Two strategies based upon multivalent expression of anti-PD-1 and anti-CTLA-4 antibodies have demonstrated this premise in vitro, in animal models, and in the clinic, with ongoing investigation. More broadly, these findings hint that immunotherapy resistance may derive from ineffective binding at the current dosing, introducing opportunities for improving drug design and delivery to tackle this issue.
Write-up by Alex Najibi, image by Lauren Hitchings
References:
[1] Mazor, Y., et al. Improving target cell specificity using a novel monovalent bispecific IgG design. MAbs 2015.
[2] Huang, L., et al. Multispecific, Multivalent Antibody‐Based Molecules Engineered on the DART and TRIDENT Platforms. Current Protocols in Immunology 2020.
Meet the researcher
This week, we had the privilege to hear from both featured teams. Below are the answers of Bradley Sumrow (co-first author) and Paul Moore (senior author) on “Development and Preliminary Clinical Activity of PD-1-Guided CTLA-4 Blocking Bispecific DART Molecule”.
What prompted you to tackle this research question?
BS: The team undertook development of MGD019 with the goal of addressing unmet medical need and ultimately delivering a potentially improved therapeutic option for advanced cancer patients. The tremendous advances achieved with combinatorial blockade of PD-1 and CTLA-4 have been tempered by significant intolerability and/or ineffectiveness in many patients. We purposefully designed this investigational agent to exploit these well validated checkpoint pathways utilizing a novel approach with the hope of achieving an improved therapeutic and safety profile.
PM: From a technical standpoint, we were motivated to determine whether a bispecific antibody-based approach could be applied to provide dual blockade of the PD-1 and CTLA-4 inhibitory pathways with activity at least as good as that achieved by the mAb combination. Furthermore, we set out to determine whether we could develop a molecule with a safety profile similar to that of anti-PD1 mAb therapy alone, but with the biological and therapeutic activity achievable with the combination of anti-PD-1 and anti-CTLA-4 mAbs.
What was the most surprising finding of this study for you?
BS: Prior to initiation of the first-in-human study, we were very encouraged by the overall preclinical data. With respect to safety, for example, the GLP toxicology results (with no adverse clinical signs noted at doses up to 100 mg/kg) compared favorably to those reported preclinically for the ipilimumab and nivolumab combination. Personally, I have been most pleasantly surprised, to date, to see this preclinical promise translate directly to patients in the clinic with encouraging tolerability, antitumor activity in typically unresponsive cancer types, and pharmacodynamic evidence of CTLA-4 and PD-1 blockade observed.
PM: After examining several bispecific formats, we were pleased that MGD019 could maintain full blockade of PD-L1 interaction with PD-1-expressing cells and the cellular interaction of CTLA-4 with its ligands, providing effective reversal of T cell inhibition imparted by either pathway. What pleasantly surprised me was the enhanced ability of MGD019 (approximately 100-fold) to block CTLA-4 ligand interaction on PD-1/CTLA-4 dual-expressing cells, relative to that achieved by the combination of anti-PD-1 and anti-CTLA-4 mAbs. This indicates MGD019 has the potential to impart more effective CTLA-4 blockade than the combination of anti-PD-1 and anti-CTLA-4 mAbs in cancer patients where PD-1/CTLA-4 dual-expressing cells are more abundant.
What was the coolest thing you’ve learned (about) recently outside of work?
BS: As we have all been adjusting to the “new norm” during the pandemic, I’ve been particularly impressed with resiliency of our children as they adapt to virtual learning, disruptions to their usual activities, etc. My 8-year-old son, who is a very active and inquisitive young man, took up chess classes and began participating in online tournaments. Unbeknownst to me, the popularity of chess worldwide has exploded amidst the pandemic, and now on a routine basis I’m reminded how seamlessly he can beat his old man.
PM: After becoming a US citizen last year, a significant and “cool” thing I was able to do recently was partake in the November 2020 election. Having left Scotland in 1991 to do a post-doc here in the US, it is actually the first time I have been able to vote in about thirty years. It was particularly nice to vote alongside my oldest son, as it was also the first election he was eligible to vote in.
Below are the answers of Yariv Mazor and Simon Dovedi, both senior authors on the paper “Design and efficacy of a monovalent bispecific PD-1/CTLA-4 antibody that enhances CTLA-4 blockade on PD-1+ activated T cells”.

What prompted you to tackle this research question?
YM: Immune checkpoint inhibitors have led to a paradigm shift in the treatment of cancer. Antibodies targeting the PD-1 and CTLA-4 pathways serve today as the backbone of the expanding approaches in the immuno-oncology space. We also know that combinations of anti-PD-1 and anti-CTLA-4 agents improve the clinical benefits of each monotherapy alone and reduce the incidence of PD-1 relapsed or refractory patients. However, the elevated immune-related adverse events associated with combination therapy are dose-limiting and potentially prevent maximal efficacy in the combination setting. We therefore were determined to develop a novel bispecific antibody format that could uncouple toxicity from antitumor efficacy, with the potential to realize the full potential of combination therapy.
SD: The treatment of cancer has been revolutionised by the development of targeted immunotherapies, and a huge amount of research is ongoing to discover new molecular switches that determine the activation or inhibition of anti-cancer immune responses. So far, this field has pivoted around the blockade of PD-1/PD-L1 and CTLA-4, which has proven to be an effective combination, but unfortunately, is commensurate with increased toxicity, which limits the amount of CTLA-4 blockade that can be achieved. We were excited to see if we could improve on a conventional monoclonal antibody approach, and developed a monovalent bispecific targeting PD-1 and CTLA-4 that utilized PD-1 as an anchor on activated T cells to re-direct and enhance CTLA-4 inhibition.
What was the most surprising finding of this study for you?
YM: We know that CTLA-4 has a very rapid recycling rate; this receptor continually endocytosed into clathrin-coated pits, resulting in only a small fraction of the receptor presented on the cell surface at any given time. We were able to show that as a monovalent bispecific antibody, MEDI5752 acquired the parental anti-CTLA-4 IgG internalization profile and rapidly internalized into CTLA-4 single-expressing, and PD-1+CTLA-4+ double-expressing cells. I was most surprised to see that upon concurrent cellular binding to PD-1 and CTLA-4, MEDI5752 mediated profound downregulation and subsequent degradation of PD-1. These results represent major differentiation from other PD-1 monotherapies and mAb combination.
SD: CTLA-4 is a really interesting molecule that is rapidly internalized by T cells. There is evidence that this internalization may function to trogocytose specific proteins from the membrane of antigen-presenting cells and lead to their degradation. We found that by tethering PD-1 to CTLA-4, our bispecific antibody facilitated the internalization of PD-1 from the surface of T cells and ultimately to the degradation of the PD-1 protein. This is very different to other monoclonal antibodies that bind to PD-1.
What was the coolest thing you’ve learned (about) recently outside of work?
YM: After visiting the Yellowstone National Park, I came to learn that the re-introduction of wolves into the park in 1995 had sparked a remarkable top-down trophic cascade. In a fascinating video titled “How Wolves Change Rivers” it describes how wolves transformed not just the ecosystem of the park, but most astonishingly also its physical geography.
SD: I have been taking my turn at home schooling recently due to the COVID-19 lockdown and have been teaching my kids about Newton's Law of Universal Gravitation, and applying this to everything from how water stays in a glass to why the moon doesn’t shoot off across the solar system!



