Anti-PD-1 and anti-CTLA-4 work through distinct mechanisms, and evidence from preclinical and early clinical trials has shown that these two checkpoint blockade therapies can be even more powerful when used in combination. To determine exactly how this combination works, Wei et al. set out to uncover whether the effects of combining anti-CTLA-4 and anti-PD-1 were additive, or if distinct cellular mechanisms might be at play. Their results were recently published in PNAS.
The researchers began by investigating which immune cell populations, particularly T cells, are affected by anti-PD-1 and anti-CTLA-4 therapies. Using a mass cytometry-based systems approach, immune responses were profiled in mice bearing MC38 tumors, which are sensitive to both monotherapies and to combination therapy. Unsupervised clustering analysis revealed that the frequency of infiltrating T cells (among all infiltrating CD45+ cells) was increased following monotherapies, and was further increased by combination therapy.
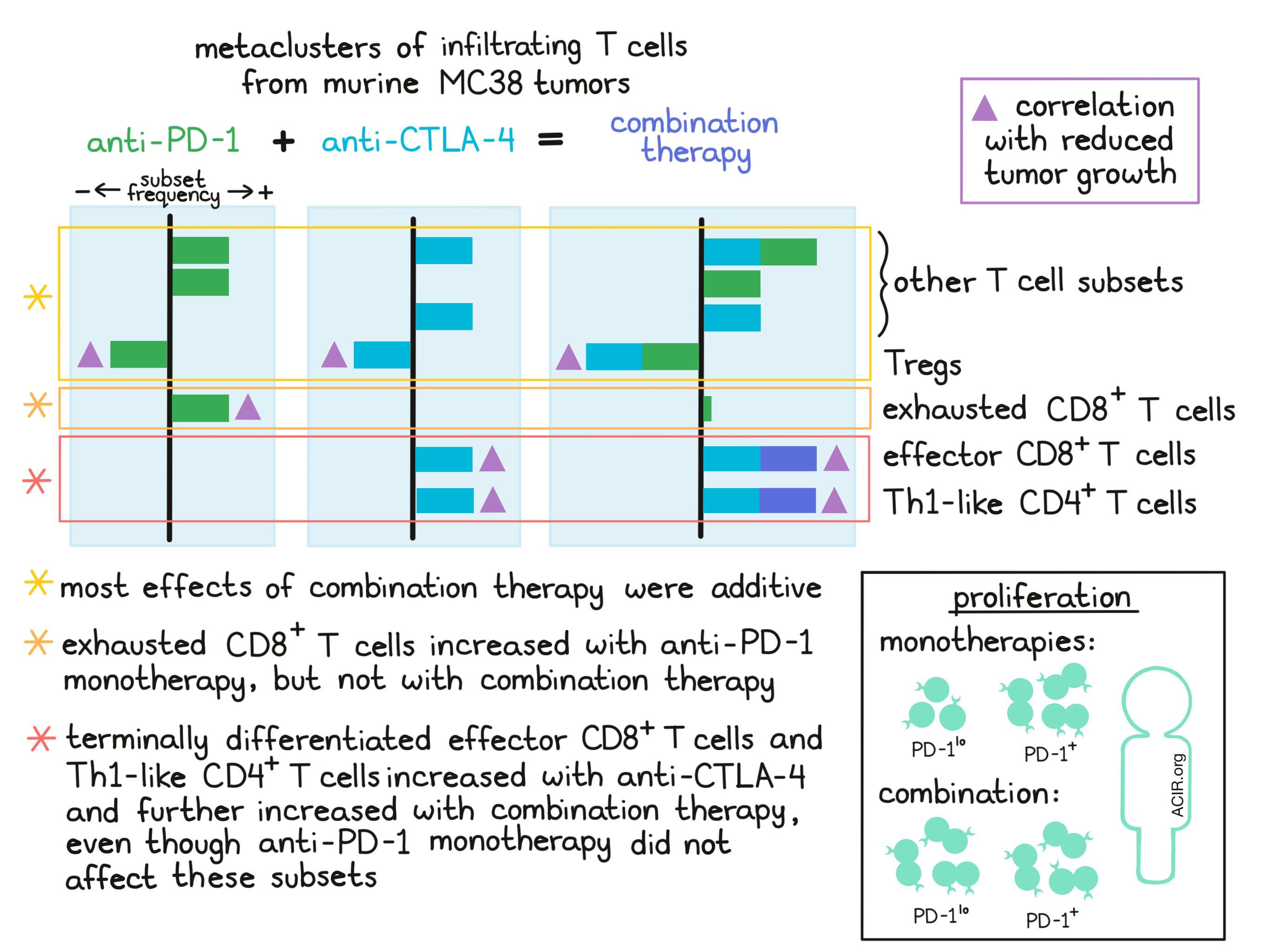
To better understand the specific subsets of T cells that respond to checkpoint blockades, the researchers applied a metaclustering approach that allowed them to analyze infiltrating T cell subsets across multiple replicate cohorts of mice. Using this strategy, they identified 14 T cell subsets, including four subsets of CD8+ T cells, three subsets of CD4+ effector T cells, and three subsets of Tregs. The frequencies of individual T cell subsets varied in response to checkpoint blockade monotherapies, and while the effects of combining anti-PD-1 with anti-CTLA-4 were mostly additive, a few notable exceptions were observed:
- While anti-PD-1 monotherapy increased the frequency of phenotypically exhausted (PD-1hiLag3+Tim3+) CD8+ T cells, combination therapy did not increase the frequency of this subset.
- Combination therapy further increased the frequency of a subset of activated, terminally differentiated, effector (PD-1+Lag3intTim3int) CD8+ T cells that was increased by anti-CTLA-4, but not by anti-PD-1.
- Combination therapy further increased the frequency of a subset of Th1-like (PD-1+ICOSintTbet+) CD4+ T cells that was increased by anti-CTLA-4, but not by anti-PD-1, suggesting that anti-PD-1 has a unique effect in the context of CTLA-4 blockade, perhaps due to upregulation of PD-1 following CTLA-4 blockade.
Further investigating the apparent mechanistic switch from the expansion of exhausted cells in anti-PD-1 monotherapy to the expansion of freshly activated cells in combination therapy, the researchers showed (using analysis of populations in size-matched tumors) that this shift was not due to the differential efficacy of the therapies. They also showed (using short-term labeling studies) that it was not due to changes in proliferation. Based on these findings and on evidence from prior studies, Wei et al. hypothesized that the observed difference is likely due to enhanced T cell infiltration and/or improved functional responses of T cells within the tumor microenvironment.
The researchers also investigated how changes in the frequencies of specific T cell subsets in response to checkpoint blockades contributed to tumor control. Most observations were in line with previous research on the mechanisms of anti-PD-1 and anti-CTLA-4 as monotherapies. For example, an increase in Th1-like CD4+ effector cells or activated effector CD8+ T cells correlated with decreased tumor volume, while an increase in a particular Treg subset correlated with increased tumor growth. Interestingly though, the frequency of exhausted CD8+ T cells correlated negatively with tumor volume in anti-PD-1 monotherapy, but positively with tumor volume in combination therapy, indicating a mechanistic difference between monotherapy and combination therapy.
Having identified mechanistic differences underlying responses to immune checkpoint blockade combination in mouse tumors, Wei et al. analyzed peripheral blood samples from patients with melanoma who were treated with anti-PD-1, anti-CTLA-4, or combination therapy. As was observed in mice, the effects of combining treatments were mostly additive, though terminally differentiated effector (TBET+EOMES+) CD8+ T cells were uniquely increased by combination therapy. Further evidence showed that while monotherapies enhanced proliferation in activated PD-1+ T cells, combination therapy induced proliferation in resting PD-1lo T cells, which could explain why it increases the frequency of terminally differentiated effector CD8+ T cells. Anti-CTLA-4 treatment induced multiple CD4+ T cell populations more effectively than anti-PD-1 treatment, although results with combination therapy were not always congruent.
To investigate the extent to which peripheral blood is useful in evaluating responses in the tumor microenvironment, Wei et al. analyzed a mass cytometry dataset of matched treatment-naive lung tumors, adjacent healthy lung tissue, and peripheral blood and identified 21 metaclusters of T cells, some of which were specific to their location. While peripheral blood T cell populations showed some resemblance to those in the tumor, T cell populations from the tumor more closely resembled populations from healthy lung tissue, indicating that resident immune cells likely contribute to tumor-infiltrating immune cells and that these cells may act more as bystanders than as tumor-specific effectors. One CD8+ T cell population and two CD4+ effector T cell populations that were not present in peripheral blood were identified in the tumor, and evidence suggested that these subsets were actively involved in an antitumor response. While the two CD4+ T cell subsets were also found in adjacent tissue and likely arose locally, the CD8+ T cell subset, which was terminally differentiated (PD-1+LAG3intTIM3int), was exclusive to the tumor, suggesting that this population arose from a systemic immune response.
Overall, Wei et al. showed that while most of the effects seen when combining anti-CTLA-4 and anti-PD-1 were additive and based on the mechanisms of each monotherapy, some mechanisms were unique to combination therapy. For example, combined checkpoint blockade altered the expansion patterns of certain T cell subsets compared the anti-PD-1 monotherapy, and offered insight into a novel role for anti-PD-1 seen only within the context of anti-CTLA-4 treatment. Additionally, specific effects of anti-CTLA-4 on certain CD4+ effector populations were observed, though the functional consequences of these are yet to be unravelled. This highlights the need to fully investigate the effects and mechanisms of combination therapy in both preclinical and clinical trials.
by Lauren Hitchings
Meet the Researcher
This week, both first author Spencer Wei and lead author Jim Allison took the time to answer our questions.

Jim Allison:
What prompted you to tackle this research question?
Our previous work showed that CTLA-4 and PD-1 therapies work through unique cellular mechanisms, as evidenced by the differences in the T cell populations enriched by either treatment. This finding fit nicely with the observation that combination of the two checkpoint inhibitors provides lasting responses in more patients than either monotherapy. It was logical to assume that the two may work in parallel, each upregulating a distinct T cell population and leading to a response that looked like the addition of the two. We were really interested to know whether that was the case or whether the combination worked with greater complexity to produce a response distinct from that seen with either monotherapy.
What was the most surprising finding of this study for you?
PD-1 therapy has been associated with acting on a population of terminally differentiated CD8+ T cells commonly referred to as exhausted because while they exhibit the proteins needed to exert cytotoxicity, they seem to have moved past their most productive times. This is not surprising because these T cells express high levels of PD-1 on the cell surface. Surprisingly, in the combination treatment, these T cells never arose at all. I’m still perplexed as to how that could occur. It really highlights how much we have left to learn about checkpoint inhibition, which is encouraging for all of the patients who have yet to see any benefit.
What was the coolest thing you’ve learned (about) recently outside of work?
I visited a winery in Italy that has been continuously operated by a single family for over 500 years. In that whole time the process by which they make their wine has remained more or less unchanged. The wine was delicious and serves as a reminder that while many things in the world could use improvement, some things are just right already.
Spencer Wei:
What prompted you to tackle this research question?
In prior work, we found that monotherapy anti-CTLA-4 and anti-PD-1 checkpoint blockade utilize distinct cellular mechanisms to enhance anti-tumor immunity. These findings aligned with the underlying basic biology (in that CTLA-4 and PD-1 act through different mechanisms), but also raised the question of how the combination of these two therapies works. Combination anti-CTLA-4 and anti-PD-1 checkpoint blockade can be more effective than the monotherapies and we wanted to understand why. It’s really critical to know how immunotherapies (and other types of therapy) interact so we can figure out which combinations are most likely to benefit patients.
What was the most surprising finding of this study for you?
I was most surprised that the relationship between tumor growth and fully exhausted CD8+ T cells completely changes in the context of combination therapy versus monotherapy. Even though these T cells are exhausted, they still contribute to the antitumor response induced by monotherapies. I expected similar biology with combination therapy, however these exhausted cells actually appear to not help at all (and actually their presence associates with increased tumor growth). We still don’t understand how these switches in biological response and role in antitumor immunity occur, but taking advantage of these types of insights is going to be essential in the next generation of immunotherapies. There’s certainly a lot of work left to be done.
What was the coolest thing you’ve learned (about) recently outside of work?
I recently learned about a “zombie”-inducing fungus, which parasitizes ants and is able to change their behavior. After proliferating in the ant, the fungus influences the ant to climb to a high place prior to dying, at which time the fungus sporulates. This is an amazing mode of propagation and just highlights how complex nature is and how little we still understand about it.



