Lymphangiogenesis, the growth of lymphatic vessels, has contradictory consequences in cancer; within the tumor, it is associated with metastasis and poor prognosis, but outside of the tumor, it can boost T cell immunity. Using this knowledge, Sasso et al. developed a cancer vaccine strategy to increase tumor control and immune memory. The preclinical data on this approach were recently published in Science Advances.
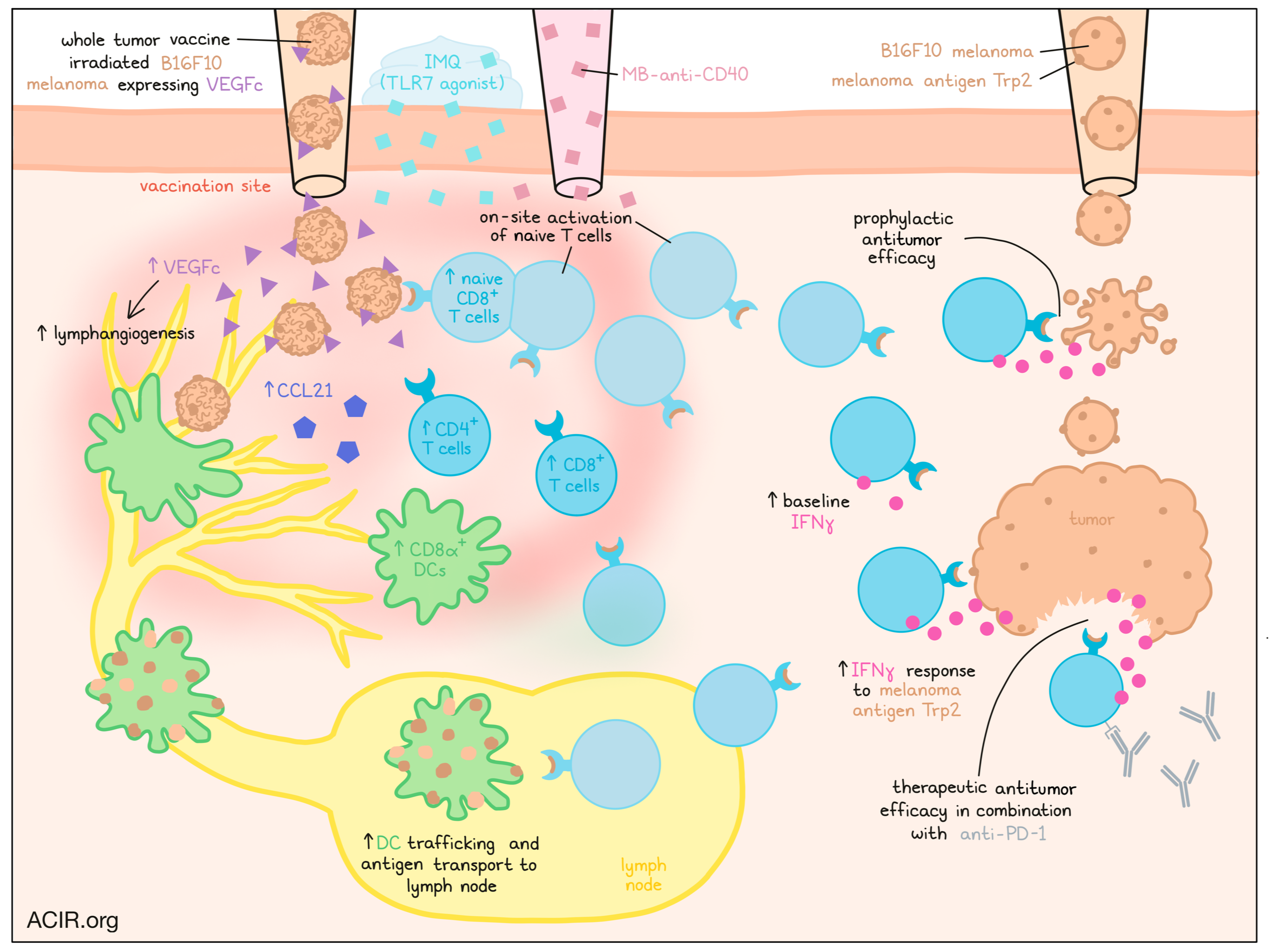
To create the vaccine, B16F10 melanoma cells were transduced to express ovalbumin (OVA) as antigen and/or vascular endothelial growth factor C (VEGFc), a known stimulator of lymphangiogenesis. After irradiation, the cells were injected intradermally into naive mice, which resulted in the growth of lymphatic vessels and infiltration of CD4+ and CD8+ T cells at the injection site in the groups that received the VEGFc vaccines. High levels of VEGFc were detected at the injection site in the first days after vaccination, and there were increased levels of CCL21, a chemokine involved in the recruitment of naive and memory T cells and dendritic cells (DCs). Similar results were found using the mouse melanoma model with the BrafV600EPten-/- (BP) cell line, except that with this vaccine, there was reduced recruitment of naive CD4+ and CD8+ T cells.
The researchers then investigated whether the lymphangiogenesis also increased lymphatic transport. They did this by injecting FITC-labeled microbeads intradermally into the inoculation site eight days after vaccination and quantifying the bead uptake by APCs in the skin and skin-draining lymph nodes (LNs). Compared to controls, the vaccinated draining LNs had higher frequencies of APCs with beads, which were migratory CD103+ and MHC-IIhighCD11b+ DCs and CD8α+ and MHC-IIlow CD11b+ LN-resident DCs. Since the beads were too big for passive drainage, these data suggested active transport by the lymphatic endothelial cells and increased DC trafficking to the LNs.
To assess whether the recruited naive T cells at the injection site could be primed to proliferate in the presence of stimuli, the TLR7-agonist adjuvant imiquimod (IMQ) was topically applied on the injection site. Mice received an adoptive transfer of naive CD8+ T cells isolated from OT-1 and pmel-transgenic mice. In control groups, few OT-1 and pmel CD8+ T cells accumulated in the draining LNs or at the site of injection, while in the VEGFc vaccination groups, high numbers of activated T cells were detected in both locations. When mice received daily injections of FTY720 (FTY) after the transfer to block S1P receptors and prevent naive and effector T cells from exiting the LNs to allow studying of local activation, both the control and VEGFc vaccination groups had high numbers of activated OT-1 and pmel CD8+ T cells in the draining LNs. However, at the injection site, high levels of activated T cells were only found in the VEGFc group, while control mice had no activated T cells. Therefore, even when T cells were depleted from the blood by FTY treatment, activated T cells were detected at the injection site of the VEGFc vaccination mice, suggesting T cell activation could occur in situ, and did not require LN involvement.
The researchers then determined whether the vaccines induced endogenous T cell responses against melanoma antigens. Vaccines created using the less immunogenic B16 cells (not-OVA) were co-treated with IMQ and a topical injection of low dose agonistic CD40-antibodies. The CD40 antibody was engineered to contain a peptide domain of placenta growth factor-2 (MB-anti-CD40) that binds to extracellular matrix, in order to retain agonistic CD40 at the injection site. Seventeen days after the co-treatment, the researchers isolated splenocytes and restimulated them ex vivo with an immunodominant MHC-I-restricted epitope from the melanoma antigen Trp2. The splenocytes isolated from VEGFc-vaccinated mice produced more IFNγ, and baseline IFNγ and IL-2 levels were also higher in this group. When VEGFc was blocked during the vaccination, lymphangiogenesis did not occur and there was a reduction in Trp2-specific IFNγ production, validating the role of VEGFc in these effects.
The experiments were repeated with the BP cell line. Since this cell line does not express detectable levels of Trp2 and other known tumor-associated antigens, the authors used whole irradiated BP cells for stimulation for the reactivity experiments. Again, higher production of IFNγ was detected in the cells from animals immunized with the VEGFc vaccine. However, in this model, the IL-2 levels were not higher at baseline.
Sasso et al. then assessed whether this vaccination strategy could prevent tumor growth. To induce lymphangiogenesis outside of the tumor, the vaccine was administered intradermally at a distant site from the tumor. The vaccine strategy was compared to another cell-based vaccine already in clinical trial testing, which uses irradiated B16F10 melanoma transduced to overexpress GM-CSF (GVAX). The researchers first compared the immune infiltrate eight days after injection. GVAX resulted in more myeloid CD11b+ DCs and CD4+ T cells at the injection site, while the VEGFc vaccination recruited more CD8α+ cross-presenting DCs and naive CD8+ T cells. Tumors were inoculated 17 days after vaccination. The VEGFc vaccination completely prevented tumor growth in all mice, while GVAX only prevented tumor growth in approximately 50% of the mice. When surviving mice were rechallenged 10 months after vaccination, the VEGFc mice showed the strongest memory response, with 50% of mice surviving.
Finally, the researchers determined the efficacy of their strategy in combination with anti-PD-1 antibodies in a therapeutic setting in which tumors were implanted before vaccination. The combination treatment (VEGFc vaccine plus anti-PD-1) delayed tumor growth and prolonged survival compared to mice receiving control vaccination and anti-PD-1. No metastases occurred in any of the treatment groups, indicating the vaccination strategy does not increase the risk of metastases.
These data suggest that establishing lymphangiogenesis at the site of vaccination is a novel strategy that can boost the efficacy of whole tumor cell vaccination. Clinical studies will have to show whether this new strategy enhances clinical efficacy, and what effects the addition of other immunotherapy strategies may have.
Write-up by Maartje Wouters, image by Lauren Hitchings



