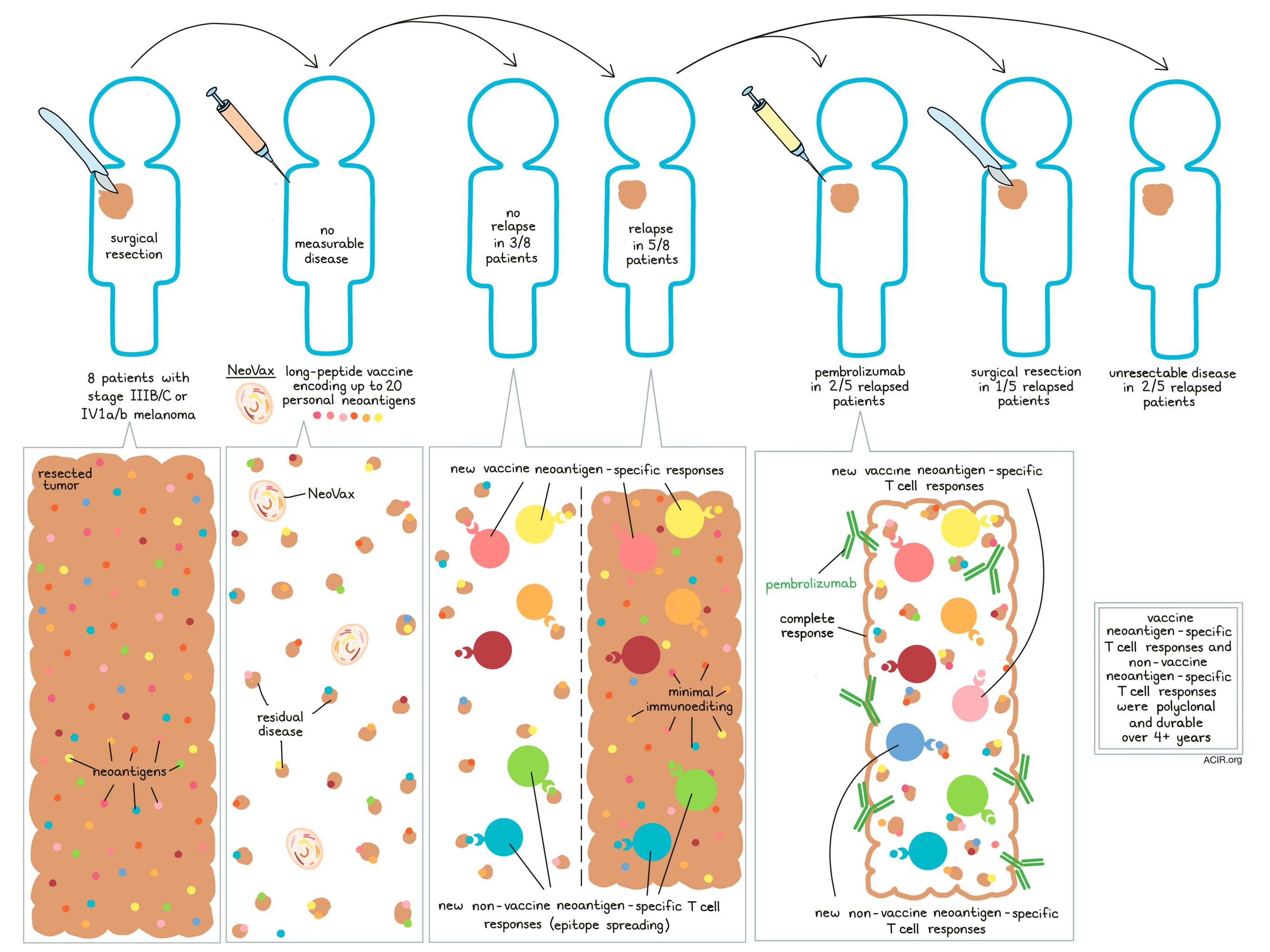
“Durable immunity is a hallmark of successful vaccination,” according to Hu, Leet, and Allesøe et al. in a paper published in Nature Medicine. The team of researchers recently followed up on the long-term effects of vaccination with NeoVax, a long-peptide vaccine that targets up to 20 personal neoantigens per patient. Their recent data extends to a median of almost 4 years post-treatment and follows the clinical outcomes and circulating immune responses of eight patients who were treated with NeoVax following complete surgical resection of stage IIIB/C or IVM1a/b melanoma.
At the last point of follow up, all eight evaluated patients were alive and six had no evidence of active disease. Five of the eight patients experienced melanoma recurrence at some point, and two of those five had a complete response following additional treatment with pembrolizumab (anti-PD-1), while another had the recurrent tumor surgically resected and has no evidence of disease. The remaining two patients developed unresectable metastatic disease.
Evaluating the mutational profiles of pre-vaccine tumor samples and samples from recurrent tumors, Hu, Leet, and Allesøe et al. found that across all five patients, 96% of mutations targeted by the vaccine persisted in the recurrent tumor, suggesting minimal immunoediting. Over time, the tumor immune environment, including the densities of cytotoxic T cells and Tregs, as well as levels of PD-1 on T cells and PD-L1 on melanoma cells, varied over time in some patients, but no clear patterns emerged.
Across all eight NeoVax-treated patients (including two who were not reported on in the previous short-term follow up paper) CD4+ T cell responses to neoantigens were more common than CD8+ T cell responses. In four patients, CD4+ T cells that were responsive to the same neoantigens could be detected ex vivo at serial time points, and showed strong ex vivo responses, demonstrating durability.
For three of these four patients, the researchers were able to directly isolate individual neoantigen-specific CD4+ T cells and characterize their transcriptional states over time at single-cell resolution. Pooling all cells, they identified four transcriptionally defined clusters, each composed of cells from all three patients. Each cluster represented a distinct T cell state identified by a specific gene signature. These four clusters represented cells that were naive-like, cytotoxic-like, activation-induced cell death (AICD)-like, or memory-like. Evaluating how these clusters shifted over the course of vaccination, the researchers found that before vaccination, the majority of cells were in the naive-like state. After priming and at early time points after boosting, cells transitioned towards the cytotoxic-like and AICD-like states, consistent with an effector response, followed by a contraction phase. At later time points, four or more weeks after vaccination, the majority of cells were in the memory-like state.
Next, Hu, Leet, and Allesøe et al. looked at vaccine-neoantigen-specific TCR clonotypes following NeoVax treatment. Across three patients tested, the researchers observed rapid and dynamic emergence of new clonotypes recognizing vaccine-neoantigens during both the priming and boosting phase of vaccination. In total, 80 unique neoantigen-specific T cell clones were identified as recurrent across various time points.
In two other patients, the researchers found that just as new clonotypes emerged after NeoVax treatment, additional new clonotypes appeared after pembrolizumab treatment. In these two patients, a majority of the clonotypes that were most prominent 16 weeks after vaccination remained most prominent and antigen-reactive one year after the initiation of pembrolizumab. Further, all of the clonotypes that were most prominent a year after treatment with pembrolizumab had been present at 16 weeks. This suggested that new clonotypes emerge both following NeoVax and following subsequent treatment with pembrolizumab, and that these emergent clonotypes are maintained long term.
Looking at whether the TCR clonotypes that emerged after vaccination were also present at the site of relapsed disease, the researchers found that in two patients who relapsed more than one year after vaccination, few or no vaccine-induced neoantigen-specific clonotypes were present in the relapsed tumors. However, in a patient who relapsed only 4 weeks after vaccination with NeoVax, several of the vaccine-induced neoantigen-specific clonotypes present in peripheral blood following vaccination were also present at the site of the relapsed tumor, suggesting that neoantigen-specific T cells were already on site when pembrolizumab treatment was initiated.
To assess whether NeoVax generated long-term memory T cell responses, the authors evaluated PBMC samples from time points up to 4.5 years after vaccination and found that the majority of CD4+ and CD8+ T cell responses against vaccine-neoantigens were maintained and were polyfunctional; persistence was further confirmed at the clonal level. In the patient who relapsed after 4 weeks and was successfully treated with pembrolizumab, vaccine-neoantigen-specific CD4+ and CD8+ T cell responses that emerged after pembrolizumab treatment remained detectable after 44 months.
Finally, while antitumor efficacy could not be directly evaluated due to the fact that patients had no measurable disease at the time of NeoVax administration, the researchers investigated epitope spreading as an indirect measure of antitumor activity in three patients. In the first patient, they found evidence of CD4+ T cell responses to non-vaccine-neoantigens that were not evident prior to vaccination. In the second patient, who also received pembrolizumab for relapsed disease, new CD4+ and CD8+ T cell responses to non-vaccine-neoantigens emerged after vaccination, and again after pembrolizumab treatment. In the third patient, who received NeoVax and later pembrolizumab for relapsed disease, no epitope spreading was observed. In the cases that did show evidence of epitope spreading, T cell responses to non-vaccine-neoantigens lasted up to over 4 years. These results suggested that NeoVax induced antitumor immune responses and epitope spreading in patients without measurable disease, and in patients with relapsed disease treated with pembrolizumab.
Overall, these results showed that NeoVax induced long-lasting T cell responses to vaccine-neoantigens, and through epitope spreading, to non-vaccine-neoantigens. Despite these durable responses, the cases of tumor recurrence suggested that NeoVax alone is likely not sufficient to prevent melanoma recurrence, highlighting the potential importance of the demonstrated synergy with subsequent checkpoint therapy. The observed insights into vaccine-induced immune responses that could help improve protocols in the future.
by Lauren Hitchings
Meet the researcher
This week, lead author Patrick Ott answered our questions.

What prompted you to tackle this research question?
We started the study in 2013 and reported initial results in 2017. Several years onwards, with substantially longer follow up of all 8 patients treated on the study and newly developed immunogenomics tools in our hands, we were eager to find out how persistent the immune responses were and whether we could characterize them using higher resolution single-cell analyses.
What was the most surprising finding of this study for you?
The number of different T cell receptor clonotypes and the fact that we were able to confirm their specificity by expressing the T cell receptors in reporter T cell lines surprised me.
What was the coolest thing you’ve learned (about) recently outside of work?
I recently started shucking Wellfleet Oysters myself. I thought it was cool that I was able to do it – but also to find out that oysters are both male and female and that the record of shucking oysters stands at 38 oysters per minute.



