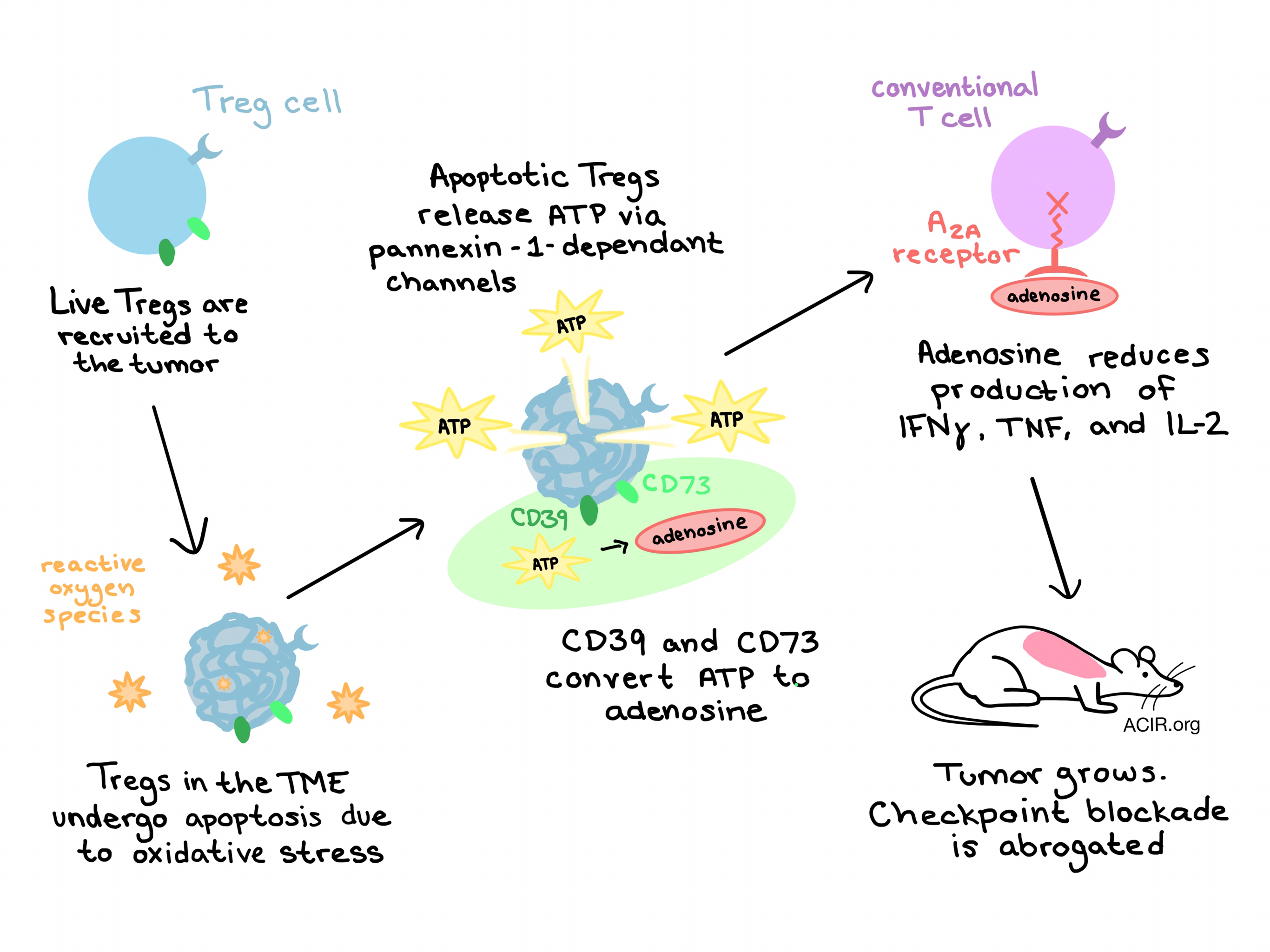
T regulatory (Treg) cells are known for their immunosuppressive role in the tumor microenvironment, but surprisingly, their death might only make them stronger. In a paper published in Nature Immunology, Maj et al. observed that while live CD4+Foxp3+ Tregs are heavily recruited to tumors, they also undergo apoptosis in the tumor microenvironment (TME) at a substantially higher rate than conventional CD4+ cells. This enhanced apoptosis was observed within human ovarian tissue as well as in several mouse tumor models.
Surprisingly, Maj et al. observed that apoptotic Treg cells also exhibited immunosuppressive abilities, including the ability to reduce the expression of IFNγ, tumor necrosis factor (TNF), and IL-2 by CD4+ and CD8+ T cells in vitro; the inhibition of IL-2 by apoptotic Tregs was even more dramatic than inhibition by live Treg cells. Administration of apoptotic Tregs to three separate therapeutic mouse models – one of spontaneous T cell immunity, one of anti-PD-L1-induced immunity, and one of adoptive T cell transfer-mediated immunity – dampened immunity and promoted increased tumor growth, confirming prior in vitro evidence of the immunosuppressive action of apoptotic Tregs. In the model of PD-L1 blockade-induced immunity, the addition of apoptotic Tregs completely abrogated the efficacy of the checkpoint blockade therapy, suggesting that apoptotic Tregs may play a role in the lack of efficacy of checkpoint blockade therapies in some patients.
Maj et al. next sought to understand the mechanism by which apoptotic Tregs suppress antitumor immunity. An interrogation of the usual suspects – PD-1, PD-L1, CTLA-4, TGFβ, IL-35 subunit EBI3, and IL-10 – however, showed that none had played a role in the apoptotic Treg cells’ mode of action. A 3-kDa molecular weight-cutoff filter, proteolytic digestion, and charcoal absorption suggested that the immunomodulatory effects were likely due to small molecules rather than larger proteins or peptides, leading the researchers to suspect adenosine, which can be produced by live Tregs from ATP via CD39 and CD73. Their suspicion was confirmed when the application of adenosine to T cells reduced production of TNF and IL-2 in T cells; blocking the adenosine receptor A2A on T cells abrogated this effect.
The team then hypothesized that CD39 and CD73 must remain enzymatically active in apoptotic Tregs and continue to mediate adenosine production. Further experiments indeed revealed that apoptotic Treg cells release a large amount of ATP through pannexin-1-dependent channels; ATP is subsequently converted to AMP via CD39 and then to adenosine by CD73. The chemical or genetic inhibition of either CD39 or CD73 in apoptotic Tregs was sufficient to restore IL-2 production to normal levels in conventional T cells.
The final piece of the puzzle for Maj et al. was to understand why Treg cells disproportionately undergo apoptosis in the first place. They first suspected that Treg cells, like conventional T cells, might be sensitive to glucose restriction, but this was not found to be the case. They next explored the fact that the TME is often rich in reactive oxygen species (ROS). In tumor-infiltrating Tregs, Maj et al. observed high mitochondrial activity and increased presence of intracellular ROS, suggesting that oxidative stress was likely the driving metabolic force behind their apoptotic behavior. Experimental oxidation with H2O2 and scavenging of free ROS confirmed this suggestion. Genetic analysis of tumor-infiltrating Tregs showed low levels of NRF2 and other gene transcripts associated with the antioxidant system, which would weaken this system and contribute to the vulnerability of Tregs to oxidative stress.
These results highlight the critical role of metabolism, by both tumor and immune cells within the TME, in promoting a pro-tumor outcome, and specifically suggest that the oxidative pathway is a metabolic checkpoint that controls the apoptotic, pro-tumor behavior of Treg cells. These findings may also indirectly explain why antibody-based Treg depletion, which could yield a sustained suppressive Treg cell apoptosis, is ineffective as an immunotherapeutic strategy, and why checkpoint blockade therapy is only successful in a subset of patients.
by Lauren Hitchings



