Responses to immunotherapy vary due to a number of factors, and according to two recent papers published in Science, the gut microbiome is definitely one of them. Both papers indicated that diversity of bacteria and the abundance of certain types of bacteria can affect patients’ response to anti-PD-1 immunotherapy for some cancer types, and supported these conclusions with mouse studies.
In one of the studies, Gopalakrishnan et al. examined both the oral and gut microbiomes of patients with melanoma prior to and during anti-PD-1 immunotherapy, and found variance in microbiome diversity and composition between patients who responded to checkpoint blockade and those who did not. Pre-therapy samples from responders showed higher diversity, which correlated later with prolonged progression-free survival (PFS).
Along the same line, Routy et al. observed that dosing MCA-205 sarcoma-bearing mice with broad-spectrum antibiotics during anti-PD-1 or anti-PD-1/anti-CTLA-4 therapy significantly compromised the antitumor effect of the treatments. An analysis of human patients who had undergone treatment with anti-PD-1 for advanced non-small cell lung cancer, renal cell carcinoma, or urothelial carcinoma revealed that patients who had also taken antibiotics (for various common infections) shortly before or during anti-PD-1 therapy had significantly reduced PFS and overall survival compared to patients who did not take antibiotics.
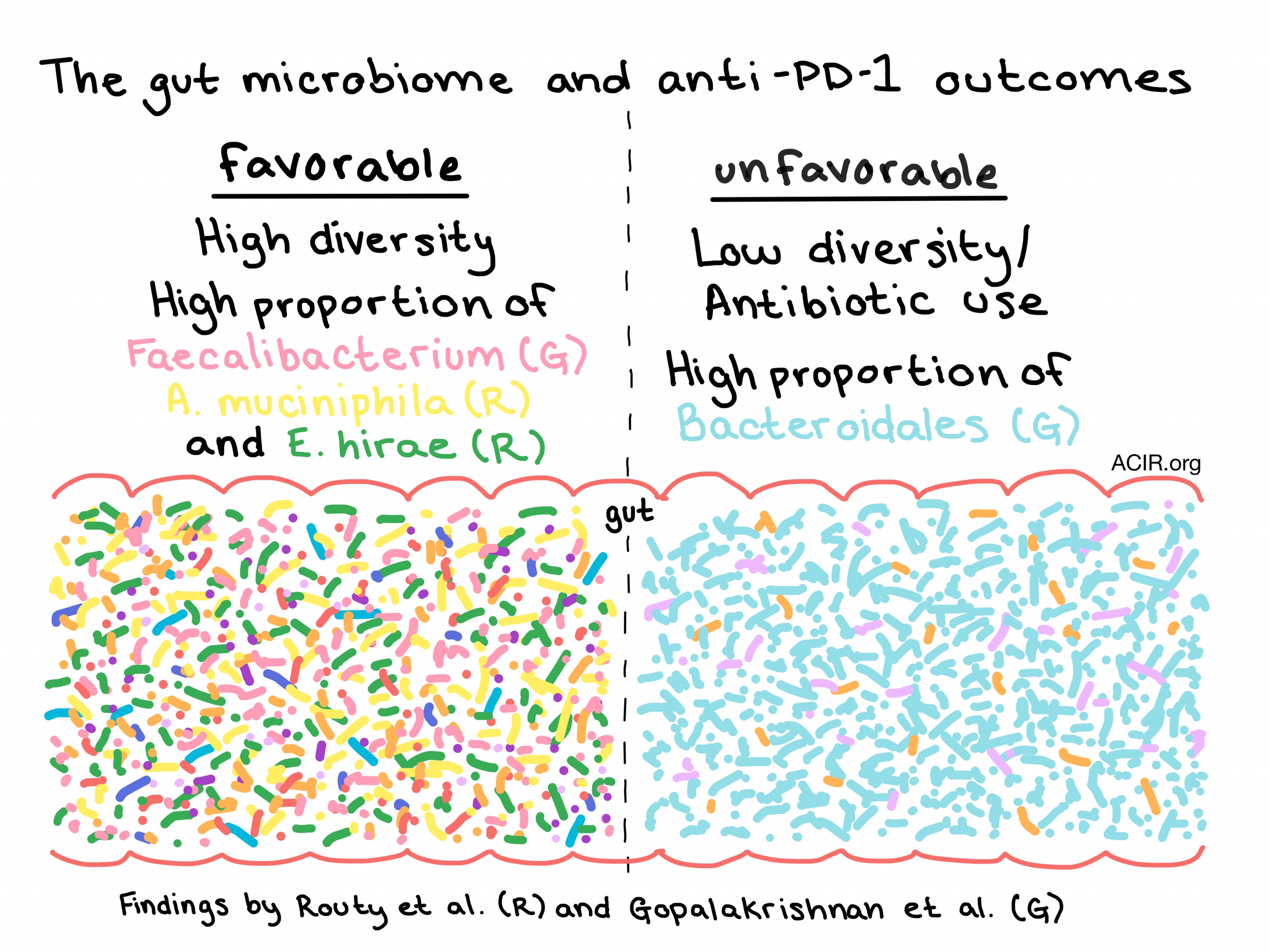
Both research teams explored the overall profile of the gut microbiome and compared anti-PD-1 immunotherapy responders and non-responders. Gopalakrishnan et al. most notably observed that fecal samples from patients with melanoma who responded to anti-PD-1 were enriched for microbes from the Faecalibacterium genus, while non-responders were abundant in microbes from the Bacteroidales order. Prominence of Faecalibacterium specifically correlated with longer PFS, while an abundance of Bacteroidales correlated with shortened PFS. In patients with epithelial cancers, Routy et al. found Akkermansia muciniphila to correlate with clinical responses to checkpoint inhibition. Overrepresentation of this species at diagnosis was a predictor of patients who would benefit most from PD-1 inhibition. Enterococcus hirae, which has previously been reported to be associated with an immunomodulatory effect, was also observed at a higher incidence in responders.
To prove a causal, and not just a correlative link between the gut microbiome and response to checkpoint blockade, both research groups performed fecal microbiota transplantation (FMT) experiments in mice. Gopalakrishnan et al. observed that transplantation of stool from responders into germ-free mice (FMT-R mice) reduced the growth of engrafted tumors compared to transplantation of stool from non-responders (FMT-NR mice), while Routy et al. did not see a comparative reduction in the growth of tumors. Both research teams, however, saw delayed tumor growth in FMT-R compared to FMT-NR mice following PD-1 blockade. Gopalakrishnan et al. noted a higher density of tumor-infiltrating CD8+ T cells, and Routy et al. observed an accumulation of CXCR3+CD4+ T cells in tumors. Tumors in FMT-R mice from both experiments also showed upregulated PD-L1 expression, indicating the development of a hot tumor microenvironment.
To determine whether an unfavorable microbiome could be improved in mice, Routy et al. provided FMT-NR mice with an oral supplement of Akkermansia muciniphila or a combination of Akkermansia muciniphila and Enterococcus hirae. Both treatments restored the efficacy of PD-1 blockade, increased the ratio of CD4+ to Foxp3+ T cells, and induced dendritic cells to secrete IL-12 by increasing recruitment of CCR9+CXCR3+ CD4+ T cells to the tumor.
Delving into the mechanism underlying the microbiome’s contribution to the efficacy of checkpoint blockade, Gopalakrishnan et al. performed functional genomic profiling, which revealed differences in metabolic functions between responders and non-responders. Anabolic processes, including amino acid biosynthesis, were predominant in responders, while catabolic pathways were more common in non-responders. Immune profiling showed that on the systemic level, patients with favorable microbiomes had increased levels of effector CD4+ and CD8+ T cells and a preserved cytokine response to anti-PD-1 therapy, while patients with a higher abundance of unfavorable microbes in the gut had higher levels of Tregs and myeloid-derived suppressor cells in systemic circulation and a weakened cytokine response.
These two studies confirm that the gut microbiome has a role in mediating patient response to anti-PD-1 immunotherapy, and their results could quickly lead to novel clinical studies. If proven, strategies to avoid antibiotic use during checkpoint blockade therapy, support a diverse gut microbiome in patients, and supplement specific beneficial microbes could be simple to implement, and could swiftly lead to improved clinical outcomes in anti-PD-1 immunotherapy.
by Lauren Hitchings



