Elevated levels of CD4+ regulatory T cells (Tregs) are often found in human tumors and are associated with poor prognosis. However, the antigen specificity of intratumoral Tregs is not well understood. In a paper recently published in Science Immunology, Ahmadzadeh et al. analyzed the relationships of TCR sequences between intratumoral FOXP3+ Tregs, circulating CD4+ Tregs, and conventional FOXP3-CD4+ cells, as well as the specificity of intratumoral Tregs, with the ultimate goal of improving immunotherapeutic approaches.
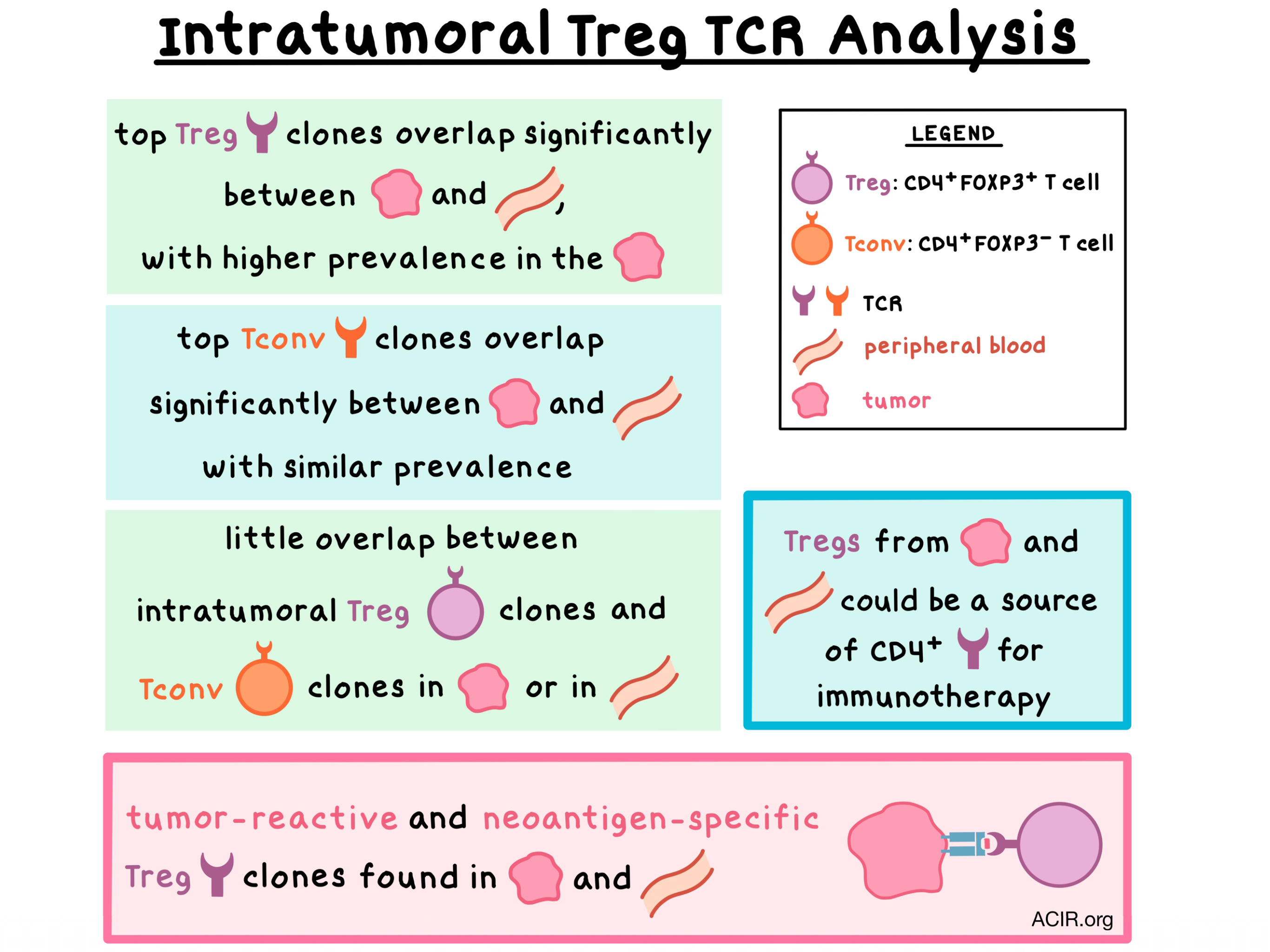
The researchers began by deep sequencing the TCRβ chains of intratumoral Tregs and conventional T cells isolated from six patients with metastatic melanoma, gastrointestinal, or ovarian cancers. Tregs exhibited a diverse TCRβ repertoire that was distinct from conventional T cells, with only a small, variable (<1 to 13%) fraction of shared clonotypes between the two cell populations. These results were consistent with previous findings from peripheral blood of healthy adults showing a small extent of overlap between the populations. The most dominant intratumoral Treg clonotypes overlapped significantly with Tregs from peripheral blood, but not with circulating or intratumoral conventional T cells. Meanwhile, conventional T cells also had a significant overlap in clonotypes between the tumor and circulation.
Intratumoral, but not circulating, Tregs, have previously been shown to be activated. Consistent with these findings, the authors found that the frequency of Tregs was higher in the tumor than in circulation, with almost 20% of intratumoral Tregs in a state of active division. The top 10 most frequent intratumoral Treg clones were much more expanded in the tumor than in peripheral blood, while no significant difference in expansion of the top clones in conventional T cells was observed between the tumor and circulation. These results suggest that the clonal expansion of the intratumoral Tregs may have resulted from tumor antigen stimulation.
With these observations in mind, Ahmadzadeh et al. analyzed the dominant intratumoral Treg clones for antigen specificity. In Tregs from one patient’s metastatic melanoma tumor (patient 3107), 6 of 11 analyzed TCRs specifically recognized the tumor, with 3 of these being among the 10 dominant FOXP3+ clonotypes. Conventional T cells from the same tumor showed 7 of 9 clones reacting to the tumor, with 3 of these being among the 10 dominant clonotypes in the intratumoral conventional T cell subset. Intratumoral Tregs from two more patients with metastatic melanoma were analyzed. In patient 3919, one Treg clone displayed tumor-specific reactivity, while in patient 4066, none of the top 10 Treg clonotypes reacted to the tumor.
Digging deeper, the researchers explored whether the intratumoral Tregs recognized neoantigens arising from patient-specific mutations. Using whole-exome sequencing and RNAseq, the team identified 163 somatic mutations in patient 3107. Utilizing peptide-pulsed autologous dendritic cells and autologous or HLA class II-matched donor peripheral blood cells transduced with Treg-derived TCRs, the authors screened 11 Treg TCR clones and found that one of them exhibited reactivity to mutated annexin A1 (ANXA1). In patient 3919, the screening revealed that one Treg TCR clone reacted to mutated (but not wild-type) CCL-5/RANTES with high functional avidity. With these experiments, the researchers demonstrated that intratumoral Tregs were reactive against patient-specific neoantigens. Interestingly, neither of these TCR clones were reactive to autologous tumor cells, possibly because in both cases RNA expression was low or absent for the gene (CCL5) or mutated allele (ANXA1).
Finally, the researchers asked if tumor-specific Tregs could also be found in peripheral blood. Analyzing the TCRβ deep sequencing data from patient 3107, they found that 6 tumor-reactive Treg TCRs (including the TCR specific for the mutated ANXA1) were found in circulating Tregs. These results suggest that peripheral blood could be a source of tumor-reactive and neoantigen-specific Tregs.
Overall, the results of this study demonstrate that the elevated levels of Tregs in the tumors are likely due to tumor antigen stimulation and the resulting clonal expansion. Intratumoral Tregs displayed a TCR repertoire that was distinct from conventional T cells but overlapped with circulating Tregs. Most importantly, the most dominant intratumoral Treg TCR clones showed reactivity to the tumor and patient-specific neoantigens. Identification of Treg specificity may inform the design of future TCR-based immunotherapies against cancer.
by Anna Scherer



