Given that it is consistently expressed by tumor cells and contributes to malignant transformation, the HPV E7 antigen is an interesting target for immunotherapy in HPV-associated carcinomas. Nagarsheth et al. previously developed a high avidity TCR that recognizes the E711-19 antigen complexed with HLA-A*02:01. The TCR-T cells containing this E7-targeting TCR were assessed in a Phase 1 study recently published in Nature Medicine.
To manufacture the TCR-T cells, autologous PBMC were stimulated with OKT3 and IL-2, after which the cells were transduced using an MSGV1 gamma-retrovirus encoding the E7 TCR. After a secondary expansion step with feeder cells, OKT3, and IL-2, cells were transfused into patients. The manufacturing time was approximately 23 days, and a median of 96% of the infused product expressed the E7 TCR.
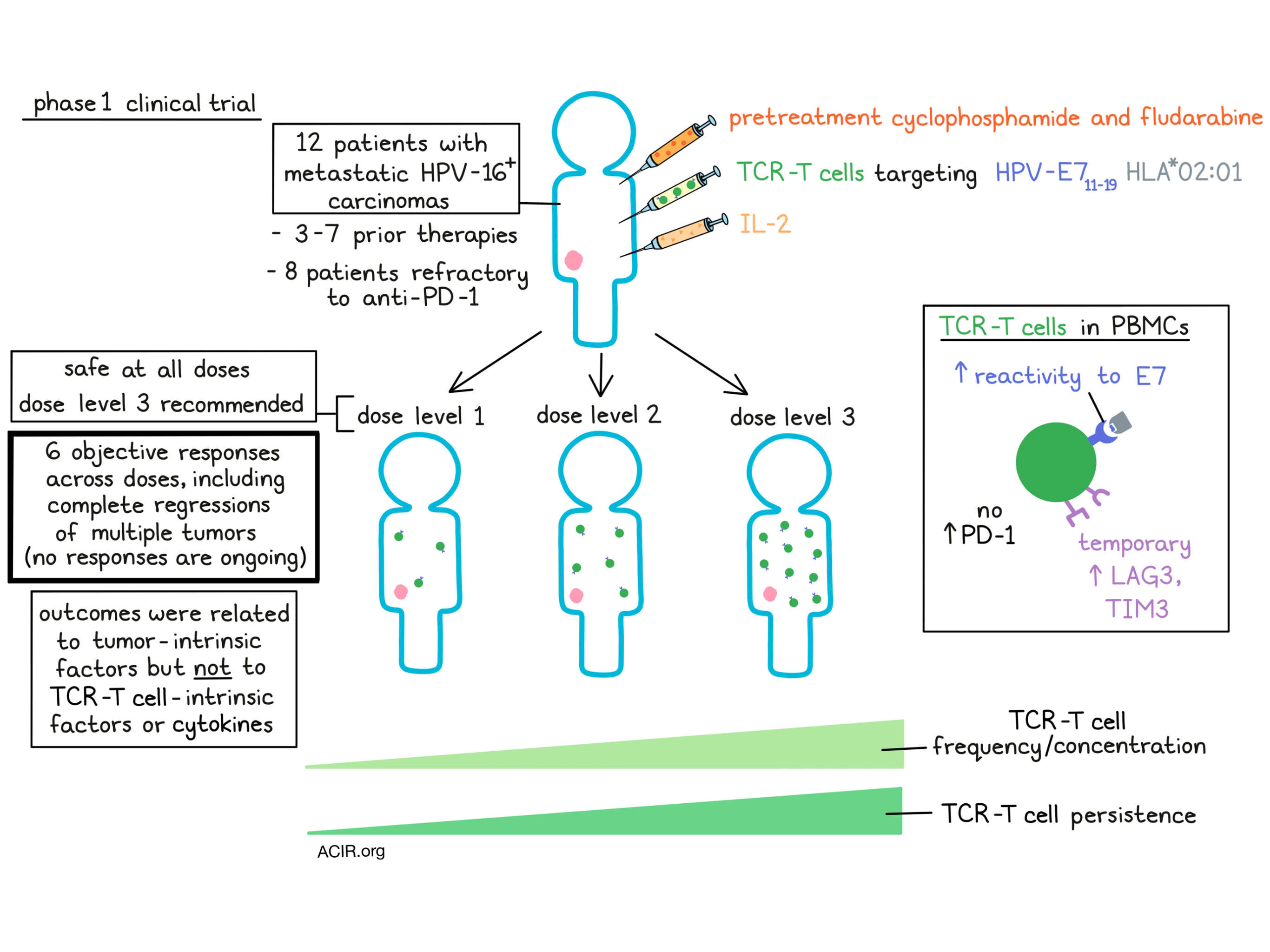
Twelve patients with metastatic HPV-16+ carcinomas (11 squamous cell carcinomas and one adenocarcinoma) were included in the trial. The primary tumor locations were uterine cervix, head and neck, anus, or vulva. Nine patients had received prior immunotherapy; eight patients received PD-1 blockade, and one patient had undergone TIL cellular therapy. The researchers conducted the study using a 3+3 dose escalation strategy to determine the maximum tolerated TCR-T cell dose. Patients were treated with 1x109 (level 1), 1x1010 (level 2), or 1x1011 (level 3) TCR-T cells. All patients received cyclophosphamide and fludarabine before infusion, and the TCR-T cell treatment was supplemented with aldesleukin (IL-2).
No dose-limiting toxicities occurred at the two lower doses. One patient in the dose level 3 group developed rapidly progressive lung metastases causing impaired pulmonary function before infusion. After infusion, cardiopulmonary complications arose that required prolonged hospitalization. Most grade 3 and 4 adverse events were known toxicities of the cyclophosphamide, fludarabine, and aldesleukin regimen. No TCR activity towards healthy tissue was observed, and the dose level 3 (1x1011 cells) was determined to be the recommended dose for a Phase 2 study.
Six of the 12 patients displayed objective responses. In some of these patients, multiple metastases regressed with durable responses of 8 or 9 months. However, no RECIST responses are ongoing. The responses were observed at all dose levels, likely due to the high starting dose.
The researchers then performed immunologic studies of the TCR-T cells in the peripheral blood of treated patients to determine whether TCR-T cell characteristics were responsible for differences in response. TCR-T cell frequency and concentration varied between patients who received different dose levels, but were not different between responders and non-responders. There was a prolonged, high persistence of the TCR-T cells, particularly in patients who received the two highest doses. After treatment, the peripheral blood T cells displayed a higher reactivity against the E7 epitope, which correlated with the TCR-T cell frequency in the sample. No antibodies against the E7 TCR were detected in the peripheral blood, suggesting low immunogenicity of the TCR.
Most of the peripheral TCR-T cells did not express PD-1, but did express LAG3 and TIM3 at the time of the infusion. This expression was temporary, as this expression was decreased at six weeks after infusion. Checkpoint molecules did not correlate with response to treatment and were not more abundantly expressed on TCR-T cells than endogenous T cells. Additionally, no strong correlations were found between therapy response and phenotypic characteristics of TCR-T cells or production of IL-2, TNF-α, IFN-γ, and various other cytokines, suggesting therapy resistance was not caused by TCR-T cell characteristics.
Therefore, the researchers evaluated whether therapy resistance was associated with tumor-intrinsic mechanisms. Available tumor samples from biopsies were analyzed using whole-exome sequencing and RNAseq, and associations between response and alterations in genes involved in antigen processing and presentation and interferon response were found. For example, some non-responding tumors had copy number loss defects in TAP1, TAP2, IFNGR1, and IFNGR2, and another resistant tumor had a nonsense mutation in HLA-A*02:01.
Comparing responding and non-responding tumors within a patient, the researchers found more clues regarding resistance mechanisms. For example, one patient had pleural disease that regressed entirely after therapy, and one metastasis that developed while the T cell compartment still contained 53% TCR-T cells. The researchers found that the new metastasis, in contrast to the pleural disease, had a mutation in HLA-A*2:01. In another patient, a chest wall tumor rapidly regressed, while a rectal tumor did not respond. Biopsies showed the presence of TCR-T cells in both tumors. However, in the non-responding tumor, there was no colocalization of TCR-T and tumor cells. A biopsy of this tumor at the time of progression showed a copy number loss of B2M and a start-loss mutation in the remaining copy of B2M, suggesting that lack of antigen presentation might be responsible for the absence of colocalization. These results indicated that tumoral pathways of resistance to TCR-T cells were associated with defects in pathways related to antigen presentation and T cell recognition and killing.
This Phase 1 study provides evidence that E7 TCR-T cells can induce clinically relevant regression of tumors expressing the E7 antigen, even in patients who previously did not respond to immunotherapy. The mechanisms of tumor resistance to this therapeutic strategy suggest early treatment and combination strategies that help overcome these barriers, such as upregulation of interferon response and antigen processing pathways, might improve the treatment’s efficacy. A Phase 2 trial with these TCR-T cells is ongoing (NCT02858310).
Write-up by Maartje Wouters, image by Lauren Hitchings
Meet the researcher
This week, lead author Christian Hinrichs answered our questions.
What prompted you to tackle this research question?
We are developing cell therapy for common cancers. HPV-associated cancers are currently incurable in the advanced stage. We decided to target E7 in these cancers because it is consistently expressed by tumors and not expressed by healthy tissues. This was a phase I clinical trial with a primary endpoint of safety, which is a necessary step in the development of any new treatment.
What was the most surprising finding of this study for you?
The treatment demonstrated clinical activity with objective tumor responses in 6/12 patients, including responses in immune checkpoint blockade-resistant cancers. Intra-patient comparison of sensitive and resistant tumors suggested that striking defects in antigen processing and interferon response are responsible for treatment resistance. This finding reveals a critical challenge for cell therapy and other types of immunotherapy.
What was the coolest thing you’ve learned (about) recently outside of work?
With the recent snow, I’ve moved from cooking steak on a fire grill to using a cast iron pan. It turns out that there is no compromise. The steaks retain all their flavor. You can also baste them to layer in more flavor



