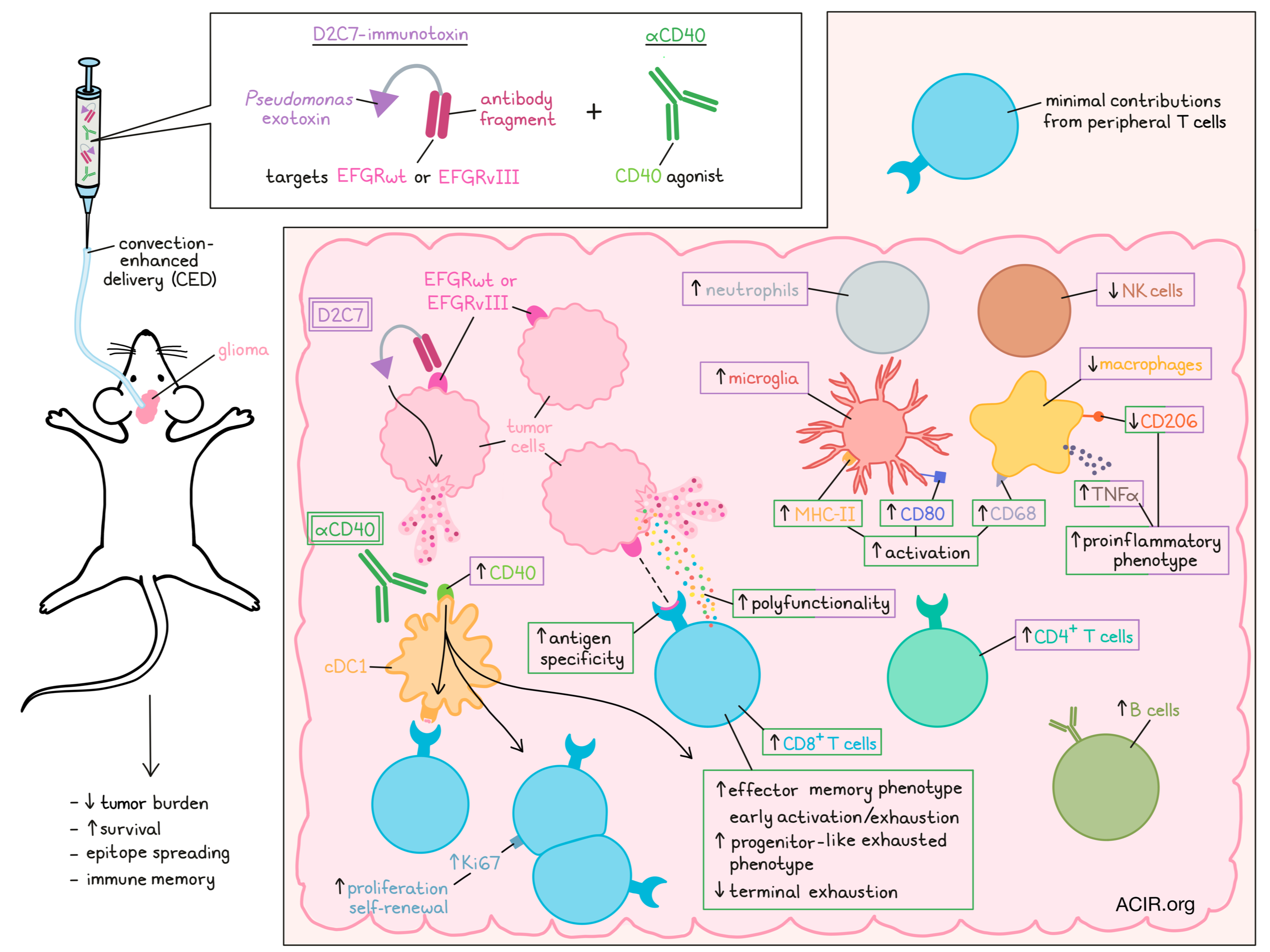
Glioblastomas (GBMs) are highly intracranially invasive and resistant to immunotherapy. In a recent phase 1 clinical trial, researchers evaluated D2C7 – an immunotoxin consisting of Pseudomonas exotoxin A and a recombinant antibody fragment that targets wild-type EGFR (EGFRwt) and mutant EGFR variant III (EGFRvIII) proteins present in GBM – in patients with recurrent grade 3 and 4 malignant glioma. While encouraging survival outcomes and radiological responses were observed in a small subset of patients, efficacy was limited. Exploring avenues to improve clinical responses, Parker et al. evaluated the possibility of using agonistic anti-CD40 (ɑCD40) to enhance antitumor immunity.
D2C7 is administered using convection-enhanced delivery (CED), which involves insertion of a catheter into the tumor mass to improve drug distribution. In order to deliver (ɑCD40) the same way, Parker et al. performed a dose-finding study that identified 100μg of αCD40 as an effective dose with limited and transient toxicity. This dose was used in further investigations comparing D2C7 or αCD40b alone, and combination therapies in the CT-2A-dmEGFRvIII-Firefly Luciferase (CT-VIII) glioma model. In this setting, the combination therapy induced tumor regression in more mice, reduced tumor burdens, and improved survival over either monotherapy. Mice that rejected tumors entirely also resisted rechallenge with parental CT-2A cells that did not express dmEGFFRvIII, suggestive of immune memory and epitope spreading. Similar results were observed in the GL261-dmEGFRvIII-Firefly Luciferase (GL-VIII) glioma model, in a model of heterogenous tumors containing a mix of CT-VIII (antigen-positive) and parental CT-2A (antigen negative) tumor cells, and in a model of metastasis/tumor cell infiltration into brain parenchyma. In models with parental CT-2A tumors, the researchers also confirmed that the contributions of D2C7 were dependent on the presence of the dmEGFRvIII target. Further, in experiments evaluating the administration route of αCD40, compared to systemic delivery, CED co-infusion showed the strongest effects on the number of survivors and duration of survival, supporting the efficacy of using this drug delivery method for both D2C7 and αCD40.
Using flow cytometry and immunohistochemistry to evaluate the impact of D2C7 and αCD40 on the immune response, Parker et al. found that at 6 days after therapy, treatment with D2C7 (monotherapy and combination) increased neutrophils and microglia, and decreased NK and macrophages. Meanwhile, treatment with αCD40 (monotherapy and combination) had minimal effects on the size of these populations, but induced activation in microglia (increased CD80 and MHC-II) and macrophages (increased CD68). In the combination-treated group, macrophages also produced more TNFα and expressed less of the anti-inflammatory marker CD206, indicative of a shift towards a pro-inflammatory phenotype.
Next looking at T cell responses, the researchers found that combination treatment increased CD4+ T cells, CD8+ T cells, and B cells, with D2C7 contributing more to the increase in CD4+ T cells and αCD40 contributing more to the increase in CD8+ T cells. Further, depletion experiments showed that the full antitumor effects of combination therapy and long-term immune protection were dependent on CD8+ T cells, but not on CD4+ T cells or B cells, establishing CD8+ T cells as the primary mediators of antitumor immunity in these models. Within tumors, most CD8+ T cells exhibited an effector memory phenotype, which was particularly increased in the αCD40- and combination-treated groups. The combination-treated group also showed the highest frequency of CD8+ T cells with an early activation/exhaustion phenotype, and the lowest frequency of CD8+ T cells that were terminally exhausted. Looking at the activation potential of exhausted CD8+ T cells (Tex), the researchers found that tumors in αCD40- and combination-treated mice contained a higher frequency of progenitor-like exhausted Tex that could be activated with anti-PD-1, and a lower frequency of terminally exhausted Tex, suggesting that these treatments limit T cell exhaustion and maintain CD8+ TILs in a more active Tex progenitor state.
To determine the contributions of intratumoral versus peripheral CD8+ T cells, Parker et al. utilized FTY720 to block T cell egress from the lymph nodes starting shortly before treatment. This had very little impact on mice treated with the combination therapy, suggesting that antitumor immunity is primarily mediated by CD8+ T cells already present in the tumor. Further, the frequency of CD8+ TILs in the brain increased in combination-treated mice regardless of FTY720 treatment, suggesting that the increase in T cells was due to on-site expansion and self-renewal, rather than from an influx of new lymph node-derived peripheral cells. In line with this, an increase in Ki67+CD8+ TILs was also observed.
In Batf3−/− knockout mice lacking cDC1s, the effects of CD40 were lost, and the effects of D2C7 and combination treatments on long-term survival were weaker than in wild-type mice. Batf3 knockout also limited the ability of combination treatment to promote progenitor-like CD8+ TILs, as most TILs in these mice were terminally exhausted.
Analyzing RNAseq data to assess treatment-induced changes in gene expression, Parker et al. deduced that αCD40 primarily mediated immune effects, like T cell trafficking, immune response, cytokine signaling, and Th1 responses. D2C7, on the other hand, was mostly involved in pleiotropic functions, including apoptosis, intracellular movements, and chemoattraction and inflammatory response. D2C7 and combination groups were also associated with pattern recognition receptor pathways, cell death through senescence, tumor growth suppression, and upregulation of CD40. Overall, there was minimal overlap between the genes modulated by D2C7 and αCD40, demonstrating distinct mechanisms of action, with D2C7 mediating tumor cell killing and promoting inflammation that supports αCD40-induced antitumor immune responses.
Additionally, more CD8+ TILs were polyfunctional following combination treatment, and a strong increase in tumor antigen-specific T cells was observed following both αCD40 and combination treatments. Polyfunctional T cells induced by αCD40 secreted mostly effector and chemoattractive cytokines, while those induced by D2C7 and combination treatments secreted a broader range of cytokines, including stimulatory, regulatory, and inflammatory cytokines. Different treatments also induced specific T cell subsets capable of secreting granzyme B, IFNγ, and MIP-1α.
Overall, these results suggest that D2C7 and αCD40 work together through complementary mechanisms that promote a pro-inflammatory immune microenvironment and support antitumor immune responses in murine gliomas expressing EGFR. Parker et al. also identified high CD40 expression in human GBM specimens, particularly in endothelial cells and around areas of necrosis, which further supports testing the addition of αCD40 to D2C7 regimens in the clinical setting. A phase 1 clinical trial of D2C7-IT with human agonistCD40 antibody administered intratumorally using CED in patients with recurrent malignant glioma is already underway.
Write-up and image by Lauren Hitchings



