Successful immune checkpoint blockade in patients with melanoma is often associated with a high mutational burden, a high level of predicted neoantigens, and an interesting side effect – vitiligo. In a study recently published in Science Translational Medicine, Lo et al. investigated whether vitiligo, an autoimmune reaction against melanocytes, contributes to the efficacy of immunotherapy.
To begin, Lo et al. evaluated data from cohorts of patients with melanoma who responded to immune checkpoint blockade despite relatively low neoantigen burdens. They found that tumor samples from these patients were enriched for gene sets related to pigmentation, including expression of melanocyte antigens that are shared between healthy cells and melanoma and have been implicated as targets in vitiligo.
The researchers hypothesized that the formation of immune responses against these wild-type melanocyte antigens contributes to antitumor efficacy. In HLA-A02+ patients with melanoma, dextramer staining revealed that expansion of CD8+ T cells specific for the melanocyte antigen MART-1 was associated with anti-PD-1 therapy across responders, but not non-responders. Interestingly, only 5 of the 13 responders developed vitiligo, suggesting that responses to melanocyte antigens may contribute to antitumor immunity even below the threshold for clinically apparent vitiligo.
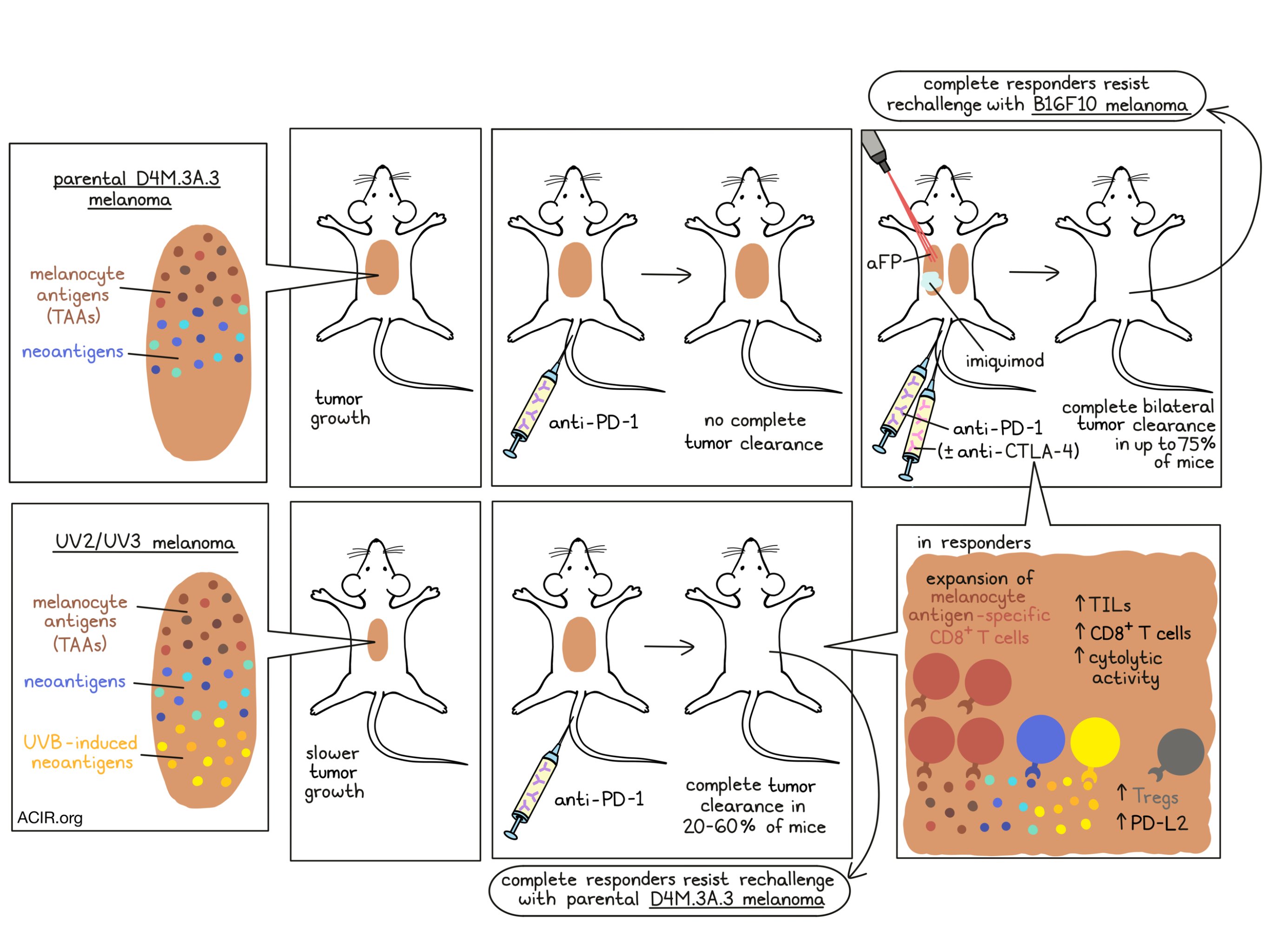
To more directly study how neoantigen and wild-type antigen recognition contribute to responses to immunotherapy, Lo et al. used a mouse melanoma cell line, parental D4M.3A.3, with a low mutation load, and subjected it to UVB irradiation to generate additional lines, including the UV2 and UV3 lines, which had similar characteristics compared to the parental line, but higher mutation loads.
When implanted into immunodeficient mice, each of these lines grew at similar rates, but when implanted into immunocompetent mice, the UV2 and UV3 lines grew more slowly, suggesting that the additional mutations and putative neoantigens contributed to antitumor immunity. Similarly, while anti-PD-1 did not induce any complete responses in mice bearing the parental D4M.3A.3 line, anti-PD-1 induced complete clearance of tumors in 20-60% of mice bearing UV2 and UV3 tumors. The UV2 line responded more strongly to anti-PD-1, and was therefore selected for use in further studies.
To investigate the contribution of responses against wild-type melanocyte antigens in this model, Lo et al. then measured T cell responses to gp100, which is enriched in melanocytes. While anti-PD-1 did not measurably affect the proportion of gp100-specific CD8+ T cells in parental D4M.3A.3 tumors, it did induce expansion of this population in UV2 tumors. Further, 6 out of 8 mice that cleared UV2 tumors following anti-PD-1 (a response that was dependent on UVB-induced mutations) rejected rechallenge with the parental D4M.3A.3 melanoma 3 months later, suggesting that the responses triggered by neoantigens induced epitope spreading to pre-existing, non-UVB-induced antigens.
To further evaluate immune responses in these animals, Lo et al. analyzed bulk tumor samples by RNASeq and found that compared to the parental D4M.3A.3 tumors, UVB-treated tumors showed strong enrichment for immune-related genes, higher overall TILs, and higher infiltrating CD8+ T cells with greater cytolytic activity. This was also accompanied by evidence of impaired CD8+ T cell function, including increased Tregs and higher levels of PD-L2.
Using the parental D4M.3A.3 tumors as a model for neoantigen-deficient, poorly inflamed, immunotherapy-resistant melanoma, Lo et al. investigated whether stimulating inflammation could improve systemic responses to wild-type melanocyte antigens and enhance antitumor responses. To this end, they tested combinations of localized laser-mediated partial destruction of subcutaneous tumors (ablative fractional photothermolysis [aFP]), topical imiquimod (a TLR7 agonist), anti-PD-1, and anti-CTLA-4 in mice with bilateral tumors. The localized treatments, aFP and imiquimod, were administered on only one flank, while anti-PD-1 and anti-CTLA-4 were delivered systemically.
While none of the monotherapies induced complete responses, various combination therapies proved more effective; unsurprisingly, the quadruple therapy had the strongest effect, inducing complete regressions in 75% of mice, followed by a triple therapy group (without CTLA-4), which induced complete regressions in 60% of mice. Generally, responses were similar on both flanks, suggesting that local aFP and/or imiquimod induced a strong abscopal effect. In 24 evaluable mice with complete responses, only one developed vitiligo and none developed any signs of gross toxicity. Triple therapy similarly improved responses in a KPC pancreatic adenocarcinoma model compared to anti-PD-1 alone.
Investigating the mechanisms underlying responses to combination therapies, Lo et al. found that imiquimod contributed to increased expression of PD-L2 on CD11c+ DCs in tumor-draining lymph nodes, increased CD8+ T cells within TIL populations, and increased granzyme B production in tumors, suggesting that it may make DCs less suppressive and improve T cell priming. Imiquimod plus aFP increased TILs and the CD8+:Treg ratio, while anti-PD-1 contributed further to infiltration, proliferation, and effector activity within tumors. In parental D4M.3A.3-bearing mice that responded to triple therapy, gp100 and TRP2 proteins were increased, as were T cells reactive to gp100, suggesting that imiquimod or aFP may have enhanced the activation of pathways related to antigen expression and presentation.
Evaluating the long-term memory responses following successful triple combination therapy, the researchers found that all surviving mice were resistant to parental D4M.3A.3. Interestingly, 38% of parental melanoma survivors and 50% of UV2 survivors were also resistant to unrelated B16F10 melanoma, which had no shared mutations. These mice were not resistant to rechallenge with wild-type KPC pancreatic tumors; however, when implanted with KPC tumor cells engineered to express 5 common melanocyte antigens, UV2 melanoma survivors survived longer than naive mice.
Finally, Lo et al. looked at a cohort of 49 melanoma patients treated with anti-PD-1 and found that sustained antitumor immune responses were associated with a highly differentiated state and with greater pigment production. Patients with melanoma who were surviving 2 years after treatment with anti-PD-1 had tumors with higher melanin scores than patients who did not survive to the 2 year mark, suggesting that immune responses to melanocyte antigens could be a contributing factor in antitumor efficacy and survival in this group.
Overall, these results show that strong responses to neoantigens can trigger epitope spreading to non-mutated tumor-associated antigens that contributes to antitumor immunity and response to checkpoint blockade. In mice, this same effect could be mimicked by inducing local inflammation, which could be relevant in a clinical setting to improve responses to checkpoint blockade in patients with low mutation burdens and poorly inflamed tumors
By Lauren Hitchings
Meet the researcher
This week, first author Jennifer Lo and lead author David Fisher answered our questions.
What prompted you to tackle this research question?
JL: Although higher melanoma neoantigen loads are associated with better responses to immune checkpoint inhibitors (ICI), they do not predict clinical benefit for individuals; for example, some patients with few neoantigens still have excellent responses to ICI. We analyzed melanoma expression datasets for clues about tumor characteristics that might compensate for neoantigen paucity and found that in low neoantigen melanomas, pigment gene expression is enriched in ICI responders over nonresponders. Interestingly, from the clinic, we knew that development of vitiligo after ICI correlates with better response to therapy. This raised the question of whether T cells targeting wild-type melanocyte antigens shared by melanocytes and melanomas (such as pigment genes) play a functional role in melanoma clearance. We were also curious about how these types of self-antigen-directed responses develop after checkpoint blockade, and how they might be generated therapeutically in patients with poor responses to current immunotherapies.
DF: I was drawn to this project by the clinical observation that many melanoma patients who respond well to ICI exhibit autoimmune vitiligo as a “side effect” of treatment. Since it is nearly impossible that distant, numerous, cutaneous melanocytes would share somatic mutations (or neoantigens) with the melanoma tumor, it suggested that autoimmune lineage targeting accompanies successful ICI. We therefore wondered if this lineage-directed immune reaction would be functionally contributing to tumor killing, rather than a mere marker of immune “activation” by ICI. Our studies here demonstrated functional involvement, and indeed a prominent role for lineage-targeting – even in tumors that contain abundant UV-induced neoantigens.
What was the most surprising finding of this study for you?
JL: We found that in melanomas with higher mutational loads, anti-PD-1 therapy led to a greater increase in the proportion of tumor infiltrating lymphocytes (TILs) targeting the wild-type melanocyte antigen gp100. I expected that with more neoantigens, checkpoint blockade would lead to expansion or recruitment of primarily neoantigen-specific TILs. However, our data suggest that epitope spreading to tumor-lineage self-antigens is actually enhanced by higher neoantigen burden. So while epitope spreading to melanocyte antigens can rescue responses to ICI in neoantigen-deficient melanomas, this epitope spreading may also be playing a complementary role to neoantigen-directed T cell activity in melanomas with high neoantigen loads.
DF: The most remarkable finding to me was the observation, by Dr. Lo and Dr. Kawakubo, that the inflammatory response induced by the presence of UV-neoantigens could be essentially replaced by a non-mutational strategy of triggering inflammation through the use of a fractional laser plus localized imiquimod. This finding suggests the potential to develop therapies that could apply to numerous cancers containing “insufficient” mutational loads to trigger an inflammatory response. Drs. Lo and Kawakubo were able to demonstrate this beyond melanoma by using a pancreatic cancer model.
What was the coolest thing you’ve learned (about) recently outside of work?
JL: Only about 200 Martian meteorites have ever been found on Earth. A couple of weeks ago, the NASA Perseverance rover brought one of these back home to Mars as part of its calibration equipment. It has been a tough year, but the incredible science (and scientists!) behind this and other breakthroughs like the COVID-19 vaccines give a lot of hope for the future.
DF: My response combines parenthood and neuroscience. I recently read the novel Home Front, by Kristin Hannah. In it, the protagonist loses her leg and suffers greatly from phantom limb pain. The writer describes how the severed nerves are confused forever, and produce painful, unresolvable signals. Our family suffered a tragedy nearly 5 years ago, when one of our children, Samuel, died suddenly upon completion of a triathlon he ran. The acute loss hit me as strikingly similar to a phantom pain – one that confuses our minds and emotions. While impossible to fully heal from this pain, the metaphor provided a helpful context in gaining strength.



