Drugs that treat cancer are numerous and diverse, and while some patients may respond well to individual drugs, many can benefit from rational drug combinations. However, testing combinations of drugs in mice can be a long, arduous, and costly process. To more efficiently test cancer drugs in mice, Tatarova et al. developed the Multiplex Implantable Microdevice Assay (MIMA), which utilizes an implantable microdevice to locally deliver nanodoses (mimicking systemic levels) of up to 18 drugs or drug combinations to spatially separate regions within a single tumor. Upon tumor harvest, these regions can be individually evaluated for changes in cell markers, phenotypes, states, and functions.
In a study recently published in Nature Biotechnology, Tatarova et al. used MIMA to asses in situ responses to seven FDA-approved drugs: olaparib (a PARP inhibitor), lenvatinib (a VEGFR-1/2/3 inhibitor), palbociclib (a CDK-4/6 inhibitor), venetoclax (a BCL-2 inhibitor), panobinostat (an HDAC inhibitor), doxorubicin (a DNA intercalating chemotherapy) and paclitaxel (a mitotic inhibitor chemotherapy). The implantable microdevice was placed into mammary tumors that developed spontaneously in immunocompetent, genetically engineered MMTV-PyMT mice, which model human breast cancer in terms of progression and heterogeneity.
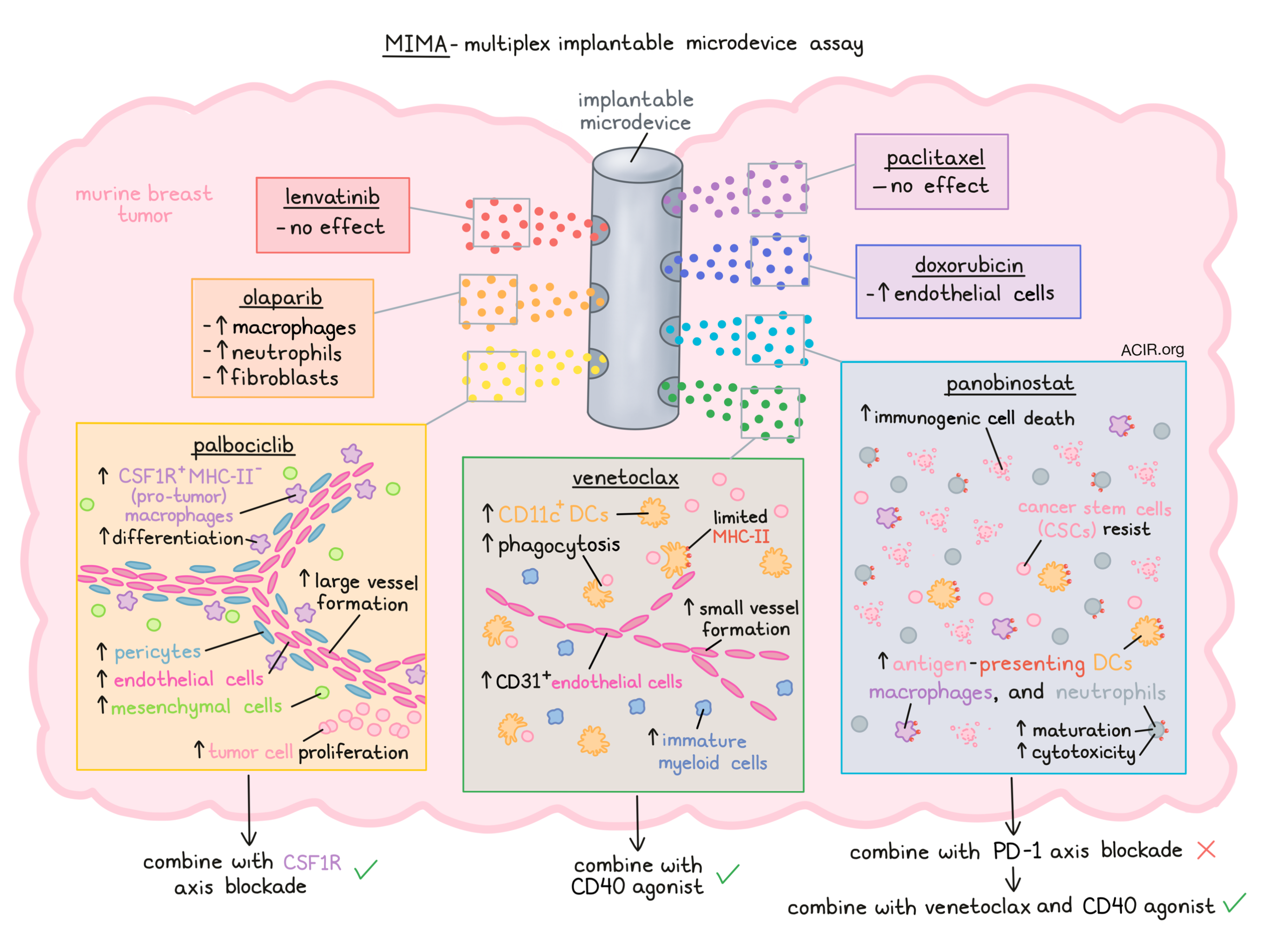
Comparing tumor tissue sections from drug-targeted areas against distant, untreated tumor tissue from the same tumors, the researchers found that lenvatinib and paclitaxel induced no detectable effects. Olparib modestly increased macrophages, neutrophils, and fibroblasts, while doxorubicin enriched endothelial cells, suggesting normalization of vasculature. Palbociclib, venetoclax, and panobinostat each produced strong changes in immune and non-immune stromal states.
To better understand the latter three of these drugs, the researchers took a closer look using extended mIHC analytics and spatial measurements. Looking first at palbociclib, they found that treated samples were enriched for several stromal types, including CSF1R+MHC-II- macrophages (pro-tumorigenic), endothelial cells, pericytes, and mesenchymal cells. Near the treatment area, macrophages were more differentiated, and in some regions, CSF1R+ macrophages were associated with contractile pericytes in branch-like patterns, suggesting that palbociclib induced the formation of large vessels. Clusters of Ki67+ neoplastic cells distant from the drug delivery site, but proximal to macrophage/pericyte networks were also observed, suggesting that the formation of large blood vessels might mediate resistance to palbociclib by contributing to an increase in tumor cell proliferation.
Based on the high CSF1R expression on multiple pro-tumor cell types, Tatarova et al. hypothesized that palbociclib might be enhanced by CSF1/CSF1R axis blockade. To test this, mice bearing EMT6 breast tumors were treated systemically with palbociclib, anti-CSF1R, or both. While neither monotherapy showed any effect, the combination reduced tumor growth.
Next looking more closely at venetoclax, the researchers observed increased CD11c+ DCs, immature myeloid cells, and CD31+ endothelial cells in the drug assay area. The endothelial cells in these samples appeared to form small blood vessels, not supported by pericytes. Further, CD11c+ DCs were aggregated into multiple spatially separate clusters and differed in phenotypes, as defined by morphology and expression of Epcam, CD45, MHC-II, and CD11b. CD11c+ DCs that were closer to the drug delivery site were found to be phagocytic, while those further out appeared unstimulated. Only a small number of DCs that were spatially associated with endothelial cells expressed MHC-II, suggesting that DCs recruited by venetoclax may be limited in their ability to present tumor antigens and stimulate T cell responses.
Based on these observations, the researchers hypothesized that venetoclax might be enhanced by a CD40 agonist to enhance APC maturation, antigen presentation, and activation potential. In mice bearing E0771 breast tumors, this combination reduced tumor growth and increased overall survival, while a combination of venetoclax and anti-PD-1 did not reduce the growth rate or improve survival.
Finally, the researchers investigated the effects of panobinostat and found that it induced immunogenic cell death, which was associated with recruitment of antigen-presenting DCs, macrophages, and neutrophils. Interestingly, neutrophils were highly abundant, and while they are not typically known for antigen presentation, 13% expressed MHC-II, suggesting that they had undergone strong phenotypic maturation.
Based on the high levels of immunogenic cell death and abundance of antigen-presenting cells in this setting, the researchers hypothesized that panobinostat would likely benefit in combination with anti-PD-1 to enhance T cell responses. In mice with EMT6 and E0771 tumors, systemic panobinostat monotherapy was found to recruit CD8+ T cells relative to stromal parenchyma, and combination with anti-PD-1 helped to reduce tumor growth and increase the duration of survival in mice. However, this treatment did not offer long-term tumor control or strong protection from rechallenge.
Digging deeper into the limited durability of panobinostat plus anti-PD-1, Tatarova et al. evaluated a list of potential biomarkers and found that ICAM1, MPO, and neuropilin-1 were localized in the proximal cell death- and neutrophil-rich region of assay, while PD-L1, galectin-3, MHC-I, and calreticulin were localized mostly on distal tumor cells. They also found that many Ly6G+ neutrophils were positive for MPO, expressed markers of cytotoxic antitumor capacity, and contributed to immunogenic cell death in the setting of panobinostat. Additionally, most neuropilin-1+ cells near the treatment region were cytotoxic, suggesting that this could serve as a biomarker for antitumor neutrophils in breast cancer.
Next, the researchers noted that nuclear expression of Sox9, which has been associated with stemness in mammary tissue and cancer, was mutually exclusive with the apoptosis marker CC3 at the border of the cell death- and neutrophil-rich region, providing direct in vivo evidence that cancer stem cells (CSCs) were resistant to therapy. Sox9 was often co-expressed with galectin-3, and 23% of galectin-3+ cells were identified as CSCs, suggesting that galectin-3 might serve a biomarker for CSCs in breast cancer.
Based on their observations of the effects of panobinostat, the researchers tested the addition of both venetoclax (to enhance recruitment of DCs to now-accessible CSCs), and anti-CD40 (to enhance DC activity and function). In mice with EMT6 or E0771 tumors, treatment with this combination therapy eliminated tumors in 100% and 85% of mice, respectively, and improved survival compared to treatment with panobinostat, venetoclax, and anti-PD-1. Similar results were observed in the MMTV-PyMT model.
Overall these results demonstrate how MIMA can be used to evaluate the effects of multiple drugs or drug combinations in the TME using a single mouse tumor model. The results of such evaluations can point to additional rational combinations for further testing.
Write-up and image by Lauren Hitchings
Meet the researcher
This week, first author Zuzana Tatarova answered our questions.

What was the most surprising finding of this study for you?
Cancer tissue can be very complex. It's composed of cancer cells themselves and cells that surround them. These surrounding environmental cells are very diverse and can have very broad functions. The most exciting result we obtained was that with a drug stimulus, the different cell subsets arranged themselves into unique shapes. Some of them resembled water–land interactions. You know, when you see a deep bay or a tree-like river delta. It seemed like nature uses the same themes over and over again. We decided to develop computational tools to process these unique spatial cell patterns and, very rapidly, we found new predictive biomarkers and new immunotherapy approaches.
What is the outlook?
One line of research will focus on how to translate the biomarkers initially discovered in mouse models of breast cancer to clinical practice, and see whether they are applicable to other cancer types. Such an approach could guide personalized treatment strategies in cancer. A second line of research will focus on how to feed the rich spatial data into mathematical models to find new biological mechanisms and targets. One exciting question would be whether we can use the spatial analyses and established immunotherapies to target resistant cancer stem cells.
What was the coolest thing you’ve learned (about) recently outside of work?
I should probably emphasize how important collaborative projects, and learning as much as possible from your mentors are. However, I must admit that my postdoctoral training also gave me a special opportunity to travel from the West Coast to the East and, for a person who does not travel that much, it was quite a breathtaking experience.



