Tumors have multiple mechanisms of immune escape, and while certain immunotherapies may help to overcome one pathway, they may have unintended consequences on another. In a study recently published in Cancer Research, Tsukamoto et al. show that both PD-1/PD-L1 blockade and IL-6 blockade have unintended consequences that might hinder their antitumor efficacy, but utilizing both therapies in combination may lead to a synergistic antitumor effect.
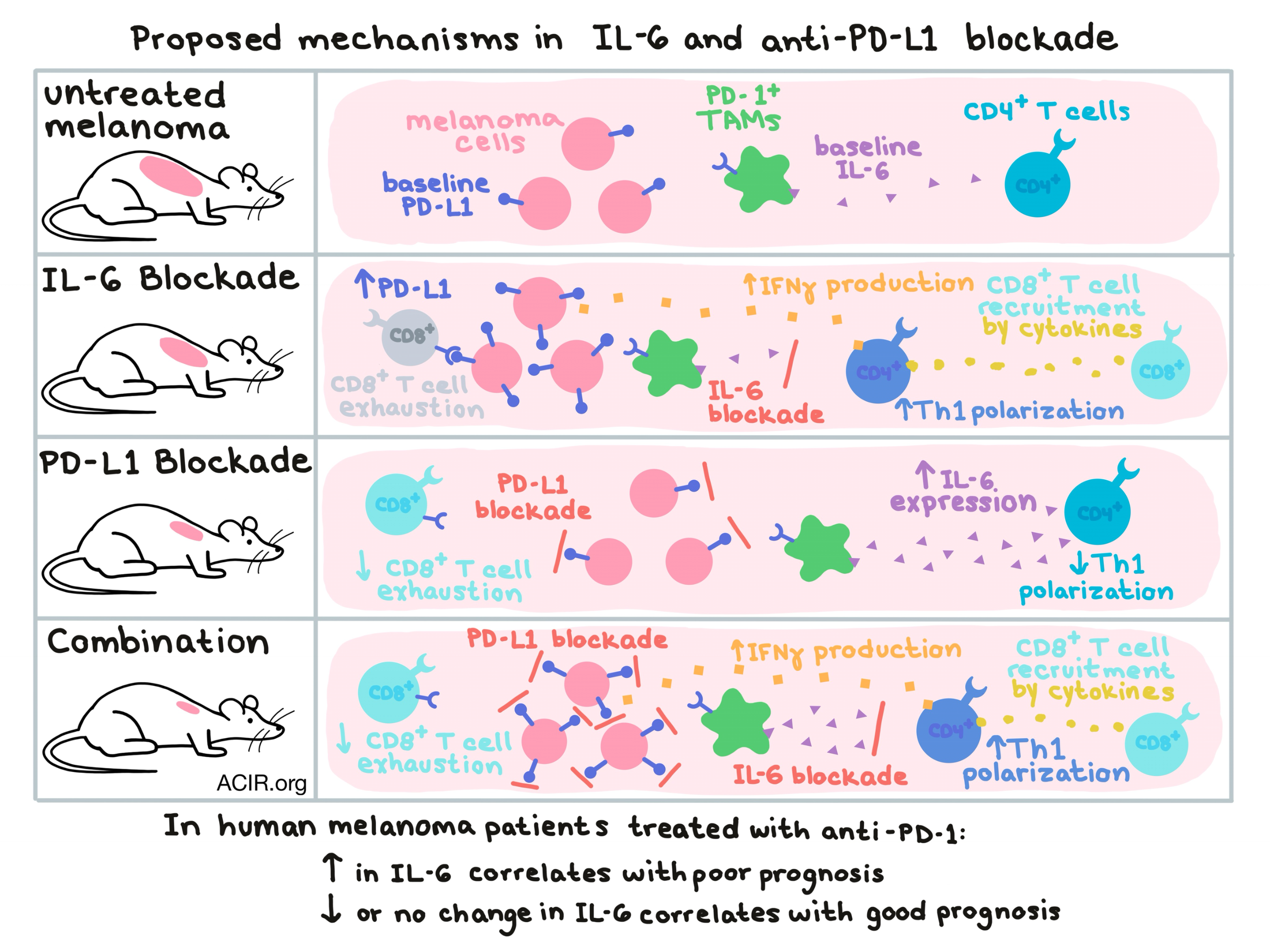
Based on previous research demonstrating that Th1 differentiation of CD4+ T cells can be attenuated by IL-6, Tsukamoto et al. tested the effects of IL-6 blockade in a murine model for melanoma. Following IL-6 blockade, the team observed an increased portion of antigen-specific, IFNγ-producing CD4+ T cells in the draining lymph node, increased CXCR3 expression by CD4+ T cells, recruitment of tumor-specific CD8+ T cells to the tumor site dependent on the presence of CD4+ T cells, decreased Th2 responses, and reduced tumor growth. Together, this data suggests that IL-6 blockade enhanced polarization towards a favorable Th1 phenotype. Despite the overall positive effect of IL-6 blockade, the increase in IFNγ production by Th1 CD4+ T cells was found to increased PD-L1 expression by melanoma cells, which likely puts a damper on the overall antitumor efficacy of IL-6 blockade.
Next, looking at PD-1/PD-L1 blockade as a target, Tsukamoto et al. examined data from melanoma patients treated with nivolumab (anti-PD-1). When the researchers examined levels of IL-6 expression, they found that although baseline levels of IL-6 had little relation to response to therapy, a rise in IL-6 levels upon treatment with anti-PD-1 correlated with shorter progression-free survival (PFS) and poor clinical outcome. Patients whose IL-6 levels remained unchanged or decreased upon treatment with anti-PD-1 were more likely to experience longer PFS and improved clinical outcomes. While only a limited number of patients were utilized in this analysis, the data identifies a rise in IL-6 upon PD-1 blockade as a possible predictive marker of non-response to therapy.
Delving deeper into the connection between PD-1, IL-6, and poor clinical outcomes in melanoma patients, the team turned again to a melanoma mouse model. In mice, anti-PD-L1 antibody increased IL-6 levels in wild-type melanoma-bearing mice, but not in IL-6-deficient mice, indicating that host cells, rather than melanoma cells, were the likely source of the increase in IL-6. The researchers identified a subset of PD-1+ TAMs as the main source of IL-6 in response to PD-L1 blockade and further showed that IL-6 production could be directly controlled by PD-1/PD-L1 ligation in this subset; blockade of the PD-1/PD-L1 axis in TAMs led to increased IL-6 production, while stimulation of the same axis led to decreased IL-6 production.
Knowing that stimulation of the PD-1/PD-L1 axis in TAMs decreased their IL-6 production, the researchers circled back to IL-6’s effect on Th1 polarization. When PD-1-stimulated TAMs (producing less IL-6) were added to a culture of activated CD4+ T cells, more CD4+ T cells produced IFNγ than when control TAMs (producing more IL-6) were added. The addition of an IL-6-blocking antibody to control TAM-treated CD4+ T cells restored differentiation towards a Th1 phenotype. In vivo, depleting TAMs reduced the previously observed increase in IL-6 upon PD-L1 blockade, and increased the IFNγ-producing CD4+ T cells in the tumor. Overall this data suggests that the production of IL-6 by TAMs impairs Th1 differentiation, and that in PD-1+ TAMs, IL-6 production can be upregulated or downregulated upon PD-1/PD-L1 blockade or stimulation, respectively.
Tsukamoto et al. hypothesized that because PD-L1 blockade caused increased IL-6, which had the negative effect of enhancing tumor PD-L1 expression in an IFNγ- and CD4+ T cell-dependent manner, and IL-6 blockade induced upregulation of PD-L1, which had the negative effect of abrogating CD8+ T cell responses, combining the two therapies might cancel out each other’s negative consequences and have a synergistic effect. They found that combining IL-6 blockade and PD-L1 blockade significantly reduced tumor growth in both OVA-expressing MO4 melanoma and CT26 colon carcinoma tumors compared to either monotherapy, though B16F10 melanoma tumors were still refractory to therapy. The synergistic effect of the dual blockade was dependent on CD4+ T cells, which did not increase in numbers, but expressed more IFNγ and CXCR3 upon treatment. Dual blockade also increased intratumoral expression levels of Ccl3/4/5 and Cxcl9/10 – genes for T cell-attracting chemokines.
While anti-PD-1 is emerging as a frontline therapy in cancer, durable effects are still limited to only a subset of patients, and biomarkers of response and additional therapies that improve its efficacy and applications are greatly needed in the clinic. Here, Tsukamoto et al. found that an increase in IL-6 upon anti-PD-1 therapy could serve as an early post-treatment marker of non-response to therapy. Additionally, they show that a blockade of IL-6 could enhance the efficacy of PD-1 checkpoint blockade, though further preclinical and clinical testing will be required to determine whether this hypothesis will hold up in the clinic.
by Lauren Hitchings



