CAR T cell therapy has proven to be an effective treatment for B cell malignancies, but treatment is often complicated by cytokine release syndrome (CRS), a severe side effect (particularly in patients with high tumor burden) that causes fever, hypotension, respiratory insufficiency, and potentially death due to spiking levels of serum cytokines. Moreover, delayed, potentially lethal neurotoxicity can follow disease clearance. Severe CRS can usually be alleviated with IL-6-blocking antibodies, but the exact mechanism underlying CRS is not fully understood. Both Giavridis et al. and Norelli et al. investigated the source of the cytokines that cause CRS, and explored possible alternative interventions to prevent or treat CRS; their papers appeared back to back in Nature Medicine.
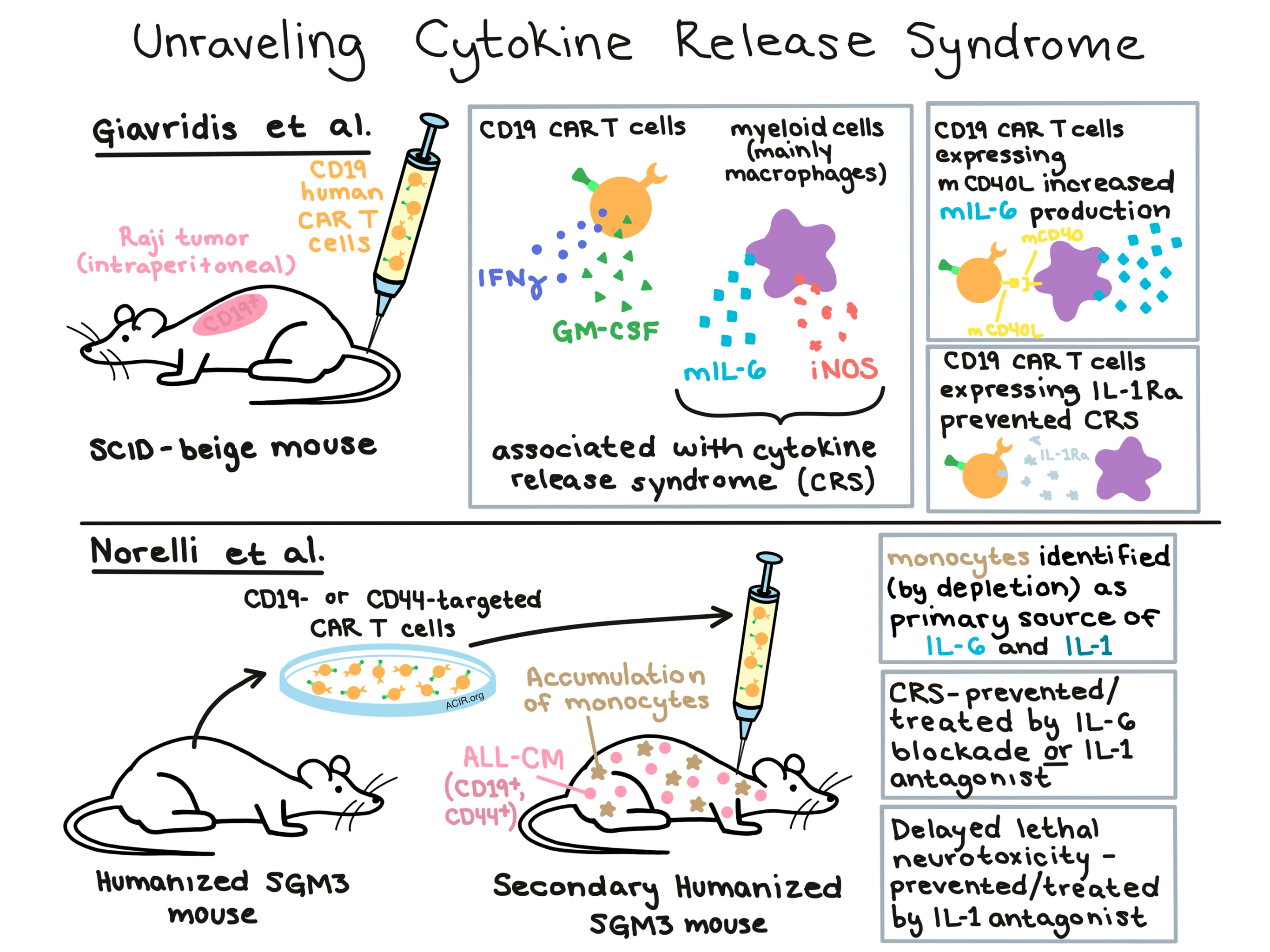
Because most mouse models do not recapitulate CRS, Giavridis et al. and Norelli et al. each developed unique mouse models. Giavridis et al. developed a model in which CD19-targeted human CAR T cells were used to treat established intraperitoneal Raji tumors in SCID-beige mice. In this model, potentially lethal CRS symptoms developed 2-3 days after infusion of CAR T cells, a cytokine profile similar to that reported in clinical studies emerged, and symptoms were responsive to IL-6 blockade.
Due to the xenogeneic nature of this mouse model, Giavridis et al. were able to easily distinguish between cytokines derived from the human CAR T cell product and those derived from the murine host immune system. While CAR T cells were found to produce cytokines like IFNγ and GM-CSF, endogenous cells were primarily responsible for the production of mouse IL-6 (mIL-6). The researchers confirmed high levels of myeloid cells (known to produce mIL-6), and identified macrophages as the main source of mIL-6.
Interestingly, mIL-6 production was only upregulated in myeloid cells that had colocalized with tumors and CAR T cells, indicating a possible interaction at the tumor site. To investigate this, the team engineered CAR T cells that expressed murine CD40L and were therefore capable of interacting with the murine CD40 receptor on host myeloid cells. These CAR T cells demonstrated enhanced symptoms of CRS even though they recruited a similar number of myeloid cells, indicating that CAR T cells interact with host myeloid cells at the tumor site, impacting CRS.
Next, the team investigated the role of inducible nitric oxide synthase (iNOS), an enzyme produced by activated macrophages, and found that only tumor-associated macrophages produced iNOS in their model. iNOS produces nitric oxide (NO) which can cause vasodilation and hypotension — symptoms associated with CRS. Symptoms of CRS could be alleviated by inhibitors of iNOS or by blockade of either IL-1 or IL-6, which are known inducers of iNOS. Lack of a synergistic effect when blocking both IL-1 and IL-6 indicated that the two cytokines utilized a common pathway.
In an effort to alleviate CRS without the need for exogenous intervention, Giavridis et al. engineered a CAR T cell that constitutively produced the IL-1 receptor antagonist (IL-1Ra). This new construct protected against CRS-associated mortality without affecting serum levels of CAR T cell-derived cytokines or impacting antitumor efficacy.
Although the model developed by Giavridis et al. effectively recapitulated CRS, it was not used to investigate the delayed lethal neurotoxicity that can appear in patients who had previously experienced CRS. In the humanized mouse model developed by Norelli et al., both of these effects were modeled. At a newborn stage, triple transgenic NSG (SGM3) mice expressing IL-3, human stem cell factor, and GM-CSF were sublethally irradiated and subsequently transplanted with human hematopoietic stem and progenitor cells (HSPCs); this strategy supported reconstitution of a human immune system and successful thymic education of human T cells. T cells from these mice were used to engineer either CD19- or CD44-targeting CAR T cells (with different endodomain variants), which were transplanted into secondary humanized SGM3 mice. The target antigen and endodomain selected for CAR T cell design both appeared to affect antitumor efficacy and CRS severity. In SGM3 mice that had been engrafted with both human HSPCs and ALL-CM leukemia cells, CRS severity and mortality following CAR T cell therapy correlated with tumor burden. Moreover, in some survivors, a sudden, sometimes lethal neurotoxicity was observed, recapitulating the late onset of neurotoxicity observed in human CAR T cell patients.
In this model, Norelli et al. noticed an accumulation of monocytes coincident with leukemia progression, and were able to determine that CRS mortality correlated with monocyte counts. Depletion of monocytes before CAR T cell infusion prevented CRS and mortality, though it had a negative effect on in vivo CAR T cell expansion and on the kinetics of leukemia clearance, indicating a possible adjuvant role for monocytes.
Like Giavridis et al., Norelli et al. found that host immune cells, not CAR T cells, were primarily responsible for producing IL-1 and IL-6, and other cytokines implicated in CRS, though in their studies, human monocytes emerged as the primary source, rather than macrophages. Interestingly, a time course study showed that IL-1 release preceded IL-6 release by about 24 hours. As expected, blocking IL-6 prevented CRS, but was unable to prevent delayed lethal neurotoxicity. Prophylactic administration of an IL-1 antagonist, however, was able to prevent both CRS and neurotoxicity without affecting the antitumor efficacy of CAR T cells. In the therapeutic setting, administration of either IL-6 blockade or IL-1 antagonist following onset of fever decreased CRS mortality, though the IL-1 antagonist had borderline statistical significance; still, only the IL-1 antagonist protected against lethal neurotoxicity and extended leukemia-free survival.
Overall, both groups showed that host immune cells, not CAR T cells, are responsible for producing the cytokines that cause CRS, both identify IL-1 as a possible alternative target to IL-6, and both present possible intervention strategies to mitigate the potentially deadly side effects of CAR T cell therapy. Finding strategies to prevent or abate CRS and neurotoxicity are critical to improving and expanding CAR T cell therapy for the treatment of cancer.
by Lauren Hitchings



