Neuropilin-2 (NRP2) is a transmembrane protein that binds ligands such as vascular endothelial growth factor (VEGF). It is expressed in several tumor types, and overexpressed in aggressive, treatment-resistant tumors, such as triple-negative breast cancer (TNBC), metastatic castration-resistant prostate cancer (mCRPC), and neuroendocrine prostate cancer (NEPC). Two recent papers from the same laboratory, published in Science Translational Medicine, described results on VEGF-specific blockade of NRP2 in these aggressive tumor types to improve immune responses and the efficacy of chemotherapy.
Prostate cancer cells can evade immune destruction by expressing PD-L1, which is seen particularly in more aggressive prostate cancers, and is correlated with poor prognosis and resistance to immune checkpoint blockade (ICB) therapy. Furthermore, these tumors express high levels of NRP2, which is also an independent prognostic factor for worse outcomes.
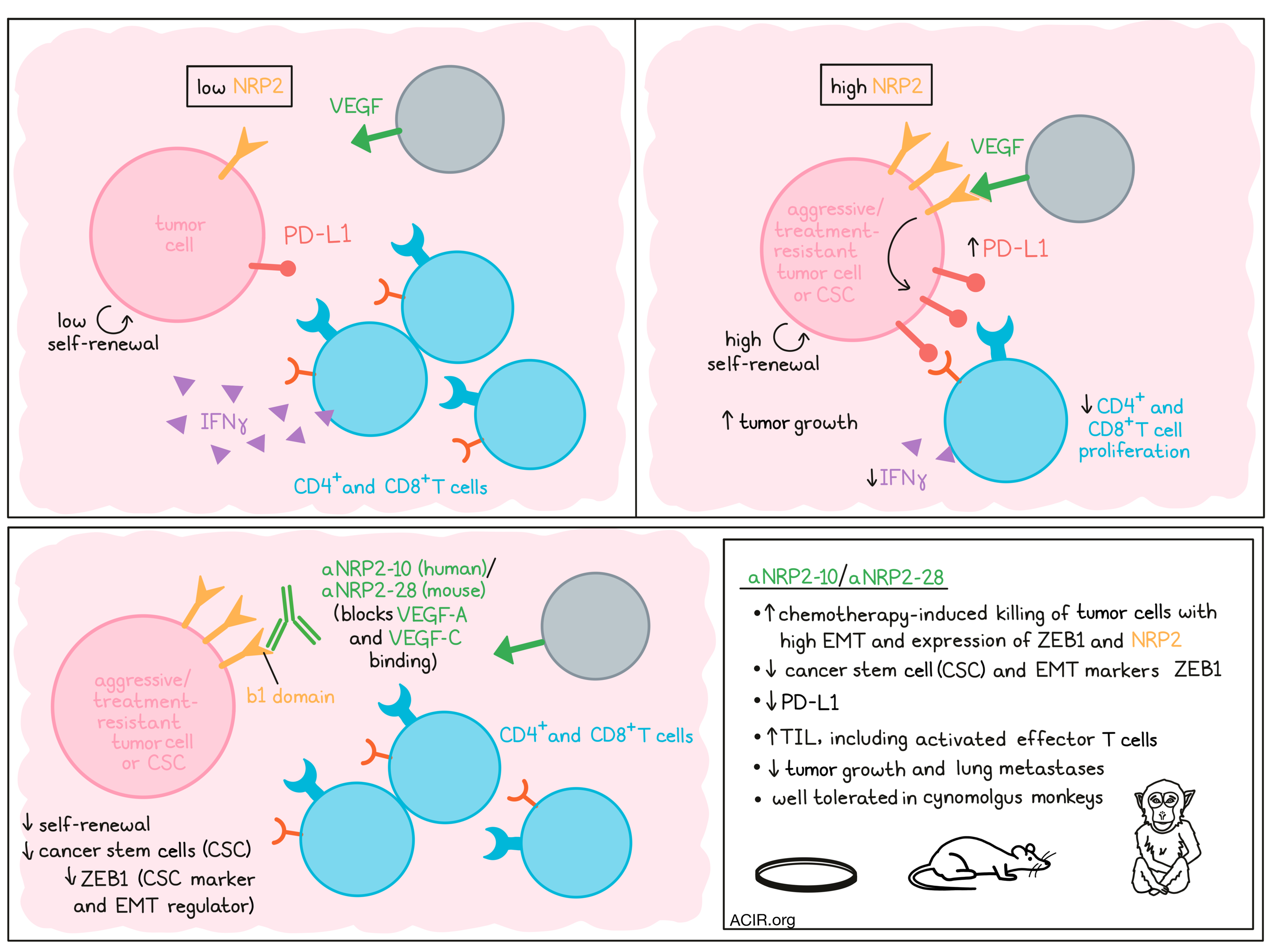
Wang et al. sorted the metastatic prostate cancer cell line PC3 based on NRP2hi and NRP2lo populations and subjected them to RNAseq. This revealed that gene networks related to the immune response were enriched in NRP2hi cells, including IFNγ signaling and CD274 mRNA (encoding PD-L1). In published human prostate cancer datasets, a positive correlation was detected between NRP2 and CD274 expression. To assess whether this correlation was causal, NRP2-deficient cells were generated using CRISPR-Cas9 or shRNA, which resulted in the downregulation of PD-L1 expression.
The researchers then investigated the immunologic effects of NRP2 expression. Coculture experiments were conducted with human peripheral blood mononuclear cells (PBMCs) stimulated with anti-CD3/CD28 and irradiated PC3 cells with or without NRP2 expression. In these cultures, the proliferation of CD8+ and CD4+ T cells was inhibited when control PC3 cells were present, while NRP3ko PC3 partially restored the proliferation of T cells and IFNγ production. When NRP2 or PD-L1 expression was restored in the KO cells, T cell proliferation was reduced, suggesting the suppression of T cell activation by NRP2 is mediated by PD-L1 expression.
To investigate a correlation between VEGF/NRP2 and PD-L1 expression in aggressive human prostate cancers, published datasets in cBioPortal were analyzed. Levels of NRP2, VEGFA, and VEGFC genes were increased in the aggressive prostate cancer subtypes mCRPC and NEPC. There was also a positive correlation between NRP2 and CD274 expression in metastatic prostate cancer samples. The NRP2hiPD-L1hi cell subsets in patients with metastatic cancer had lower androgen receptor expression and higher NEPC scores than NRP2loPD-L1lo cells, suggestive of a more aggressive phenotype.
Therapeutic targeting of NRP2 is challenging, as it functions as a receptor for multiple ligands, and only the interaction with VEGF has been associated with aggressive tumoral behavior. Therefore, Xu, Lal Goel, Burkart, et al. produced a highly specific monoclonal antibody (aNRP2-10) with a high affinity for the b1 domain of NRP2, which blocks the binding of VEGF-A and VEGF-C to NRP2, but does not block binding of semaphorin, another important NRP2 ligand.
Breast cancer stem cells (CSCs) express high levels of NRP2. The researchers sorted the BT-549 TNBC cell line into NRP2hi and NRP2lo populations. The NRP2hi cells had higher self-renewal potential than the NRP2lo cells. In vitro treatment with aNRP2-10 could significantly inhibit sphere formation of various cell lines and the self-renewal potential of CD44hiCD24lo CSC populations isolated from patient TNBC samples. To assess whether this NRP2 blockade could lower the frequency of CSCs, a transplantation experiment was performed using the murine 4T1 TNBC model. Treatment with aNRP2-28, a mouse-specific surrogate of aNRP2-10, reduced the frequency of CSCs, which was associated with a reduced expression of ZEB1, a CSC marker and regulator of epithelial-to-mesenchymal transition (EMT).
Given its effects on CSCs, which are largely chemoresistant, the researchers assessed whether aNRP2-10 could sensitize TNBC to chemotherapy treatment. aNRP2-10 treatment of 3D MDA-MB-231 cell cultures increased the sensitivity of tumor cells to cisplatin-induced killing. This was further analyzed with other cell lines, but only some of the cell lines “responded” to therapy. The responder cell lines were characterized by higher EMT scores and expression of ZEB1 and NRP2. Likewise, aNRP2-10 could sensitize TNBC patient-derived organoids to 5-fluorouracil (5-FU).
Similar increases in chemosensitization were achieved when NRP2 was downregulated using small interfering RNAs (siRNAs) in TNBC organoids, suggesting that VEGF/NRP2 signaling is a major driver of chemoresistance in these organoids. Gene expression analyses of the TNBC organoids showed that CSC and EMT markers, including ZEB1, were significantly reduced following aNRP-10 treatment, while they increased after 5-FU monotherapy.
In vivo studies with a TNBC xenograft further validated the efficacy of aNRP2-10. Antibody treatment alone did not affect tumor growth, but when combined with cisplatin, tumor growth was reduced. Gene expression analysis of the xenografts showed that CSC and EMT markers were downregulated by aNRP2-10 treatment. These effects were confirmed in another TNBC xenograft model and a patient-derived xenograft (PDX) model in combination with sub-optimal 5-FU treatment. In humanized mice with a TNBC xenograft, aNRP2-10 treatment alone reduced lung metastases.
The aNRP2 antibody was also tested by Wang et al. in comparison to anti-PD-L1 in the transgenic adenocarcinoma mouse prostate (TRAMP) model, which is resistant to ICB treatment. Established tumors were treated with aNRP2-28 or anti-PD-L1. Treatment with anti-PD-L1 did not impact tumor volume, while aNRP2-28 alone reduced tumor burden. This effect was not detected in immunodeficient NSG mice. Tumor histology analyses revealed that aNRP2-28 induced necrosis in tumors, while anti-PD-L1 did not. In the non-necrotic areas of the tumor, treatment with aNRP2-28 reduced PD-L1 expression, and there was an increase in tumor-infiltrating lymphocytes (TIL), including activated effector T cells, suggesting the tumor immune environment turned from “cold” to “hot”.
The therapeutic effects of aNRP2-10 were also assessed in the human prostate cancer setting, using human NEPC patient-derived organoid models. In this model, treatment reduced PD-L1 expression, and increases in tumor cell killing were observed when tumor organoids were cocultured with activated PBMCs.
Finally, a toxicity study performed by Xu, Lal Goel, Burkart, et al. in cynomolgus monkeys showed that aNRP2-10 was well tolerated, with no observed adverse effects at the highest dose tested.
In conclusion, these two studies showed the benefits of specifically targeting NRP2 to block VEGF signaling in aggressive cancer types, inducing antitumor immune responses in cold tumors, and targeting CSCs in breast cancer to improve the efficacy of chemotherapy. These results set the stage for testing various combination strategies with this NRP2/VEGF-targeting antibody in the clinical setting.
Write-up by Maartje Wouters, image by Lauren Hitchings.



