Pancreatic ductal adenocarcinoma (PDAC) responds notoriously poorly to treatment, including immune checkpoint blockade; combination chemotherapies are the standard of care, but clinical responses remain deficient. Recently, studies in murine PDAC models improved treatment efficacy by combining chemotherapy with a CD40 agonist antibody and immune checkpoint blockade, a strategy that has now advanced to in-patient therapy. Padrón, Maurer, and O’Hara et al. report in Nature Medicine on the combined results of phase 1b/2 trials of nivolumab (anti-PD-1, nivo), sotigalimab (CD40 agonist antibody, sotiga), or both along with gemcitabine/nab-paclitaxel chemotherapy (chemo) in 105 patients with first-line, metastatic PDAC.
In the phase 2 PRINCE trial, patients were randomized into three treatment arms: nivo/chemo, sotiga/chemo, or sotiga/nivo/chemo. In 28-day cycles, patients received intravenous gemcitabine/nab-paclitaxel days 1, 8, and 15, nivo on days 1 and 15, and sotiga on day 3, as specified per arm. Between cohorts, patients shared baseline characteristics (median age 60-63, 78-89% white, 74-79% diagnosed stage IV disease) and tumor features (PD-L1 tumor expression, KRAS, SMAD4, and TP53 expression). Prophylactic steroids were not permitted prior to chemotherapy. To characterize immune responses over the course of the study, the team collected patient blood samples and tumor biopsies before and during treatment.
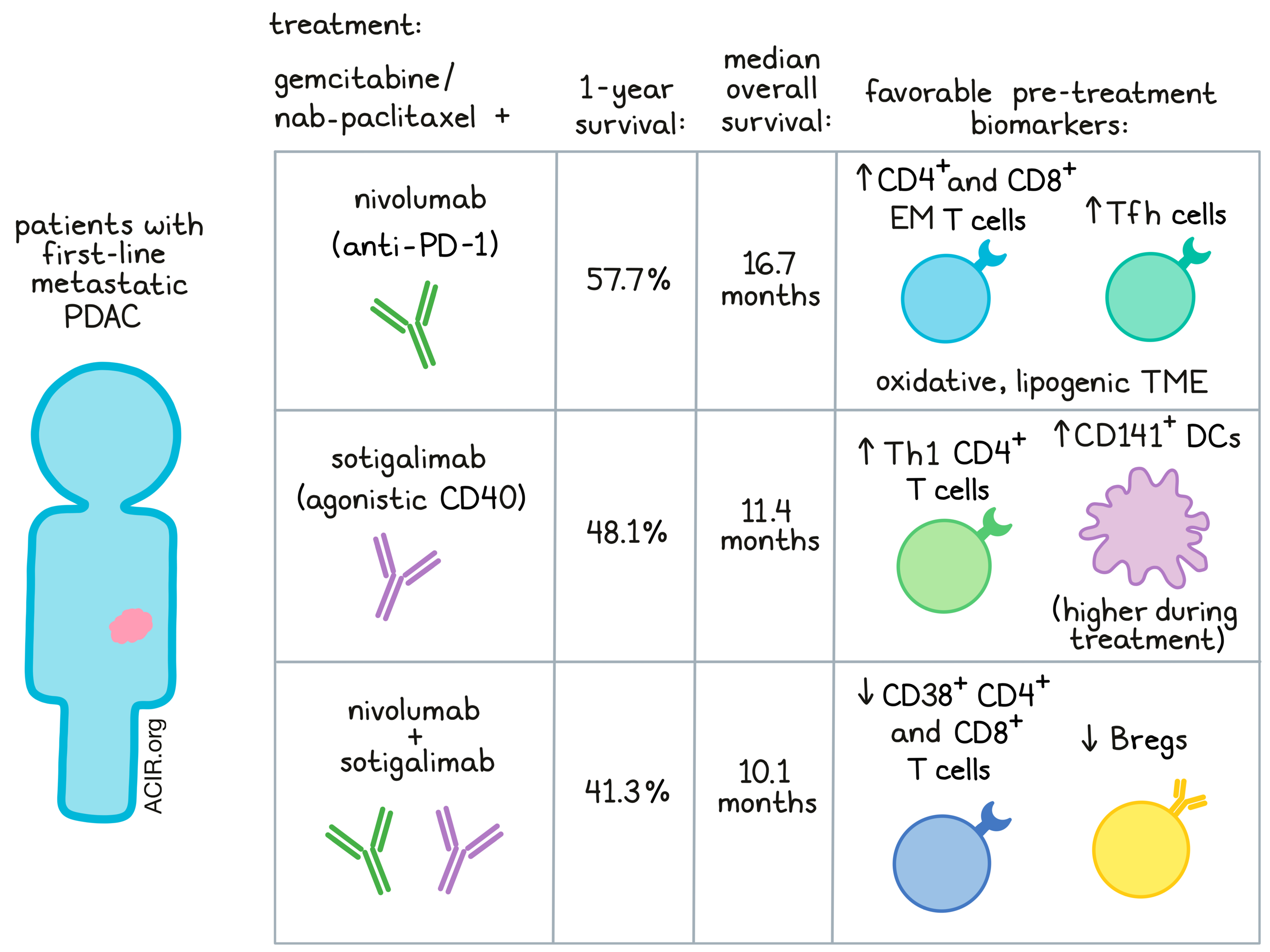
Only the nivo/chemo arm met the primary endpoint, improvement in 1-year OS rate compared to a historical chemotherapy cohort, with 57.7% versus 35% OS and a 16.7-month median OS. The sotiga/chemo and sotiga/nivo/chemo groups had 1-year OS rates and median OS of 48.1%/11.4 months and 41.3%/10.1 months, respectively; these results were not significantly different from the control group. Treatment-related adverse events occurred in almost all patients (98%) and were consistent among groups. Notably, the nivo/chemo group had the lowest rate of cytokine release syndrome (0% nivo/chemo vs. 24% sotiga/chemo and 34% sotiga/nivo/chemo; most CRS events were below Grade 3, and there were no Grade 4 or 5 events), although a higher proportion of patients in this group discontinued study due to adverse events.
Importantly, the researchers interrogated systemic and tumor features following treatment, with the goal of identifying biomarkers for treatment efficacy. RNA sequencing, CYTOF, multiplex IHC, and serum protein profiling were employed. Broadly, all treatment groups increased proliferation and activation of circulating T cells, along with serum cytokine (e.g., IFNγ) and chemokine (e.g., CXCL9, CXCL10) levels. Nivo-containing groups decreased PD-L1 tumor expression over treatment.
The team next turned to specific biomarkers associated with OS in each treatment arm. In nivo/chemo patients, pretreatment blood frequencies of effector memory CD8+ T cells expressing PD-1 and Tbet and antigen-experienced (PD-1+CD39+) effector memory CD4+ T cells expressing CTLA-4 and ICOS associated with enhanced survival. Notably, on-treatment circulating T follicular helper cell frequencies correlated most strongly with improved survival in this arm. In the tumor microenvironment, multiple gene expression signatures were related to survival outcomes, including metabolic pathways. For example, an oxidative, lipogenic tumor microenvironment was associated with better patient survival. On the other hand, gene signatures for TNFα, TGFβ, and NFκB signaling linked to poorer survival.
Interestingly, the biomarkers predictive of survival in the sotiga/chemo group diverged significantly from those found in nivo/chemo response. Here, Padrón, Maurer, and O’Hara especially considered antigen-presenting cell markers, based on CD40’s known mechanism of action and earlier findings from mouse models. In the sotiga/chemo arm, higher pretreatment frequency of cross-presenting (CD1c+CD141+) DCs, B cells, and antigen-experienced CD4+ T cells in blood related to improved survival. Similarly, on-treatment frequencies of circulating CD141+ DCs, conventional DCs, and Th1 CD4+ T cells were associated with better survival outcomes. In the tumor, CD4+ T cell gene signatures, particularly expressing Th2, Th1, and IFNγ, connected to improved survival.
Although the blood and tumor biomarkers relating to treatment efficacy largely differed between the nivo/chemo and sotiga/chemo groups, circulating IL-6 and tumor-expressed TGFβ aligned with reduced survival in both. However, the authors found little overlap between either of these groups’ biomarkers and those of the sotiga/nivo/chemo arm. In patients treated with sotiga/nivo/chemo, specific biomarkers associated with longer survival included lower frequencies of activated (CD38+) non-naive CD4+ and CD8+ T cells and CCR7+CD11b+CD27- B cells – potentially a regulatory B cell phenotype. Interestingly, circulating CD8+ T cells did not appear positively associated with response in any arm, perhaps pointing to a unique role of CD4+ T cells in the PDAC TME.
In summary, this trial and the extensive correlative data suggest that combination chemo-immunotherapy may provide value in treating PDAC, showcasing improved clinical responses and extended OS compared to a chemo-only cohort. The authors postulate that a particular treatment combination may not be appropriate for all PDAC patients; rather, the pre-treatment biomarkers identified here could lend relevance to one approach over the others, potentially attributable to the different mechanisms of action of these therapies. Additional patient trials combining response data with local and systemic immune characterization may continue to shed light on optimal treatment combinations and accelerate therapeutic development for refractory diseases such as PDAC.
Write-up by Alex Najibi, image by Lauren Hitchings




