Infection with human papilloma virus (HPV) is linked to the vast majority of cervical cancers, and while the widespread adoption of prophylactic vaccines against HPV has promised to reduce instances of cervical cancer going forward, the options remain limited for those who currently have HPV-associated premalignant or malignant lesions. In a recent study, Hillemanns et al. evaluated the use of a DNA-based, antigen-presenting cell-targeted therapeutic vaccine to treat patients with HPV+ high-grade cervical intraepithelial neoplasia (CIN) – a precursor to cervical carcinoma. The promising results of this first-in-human, multicenter, phase I/IIa clinical trial were recently published in Clinical Cancer Research.
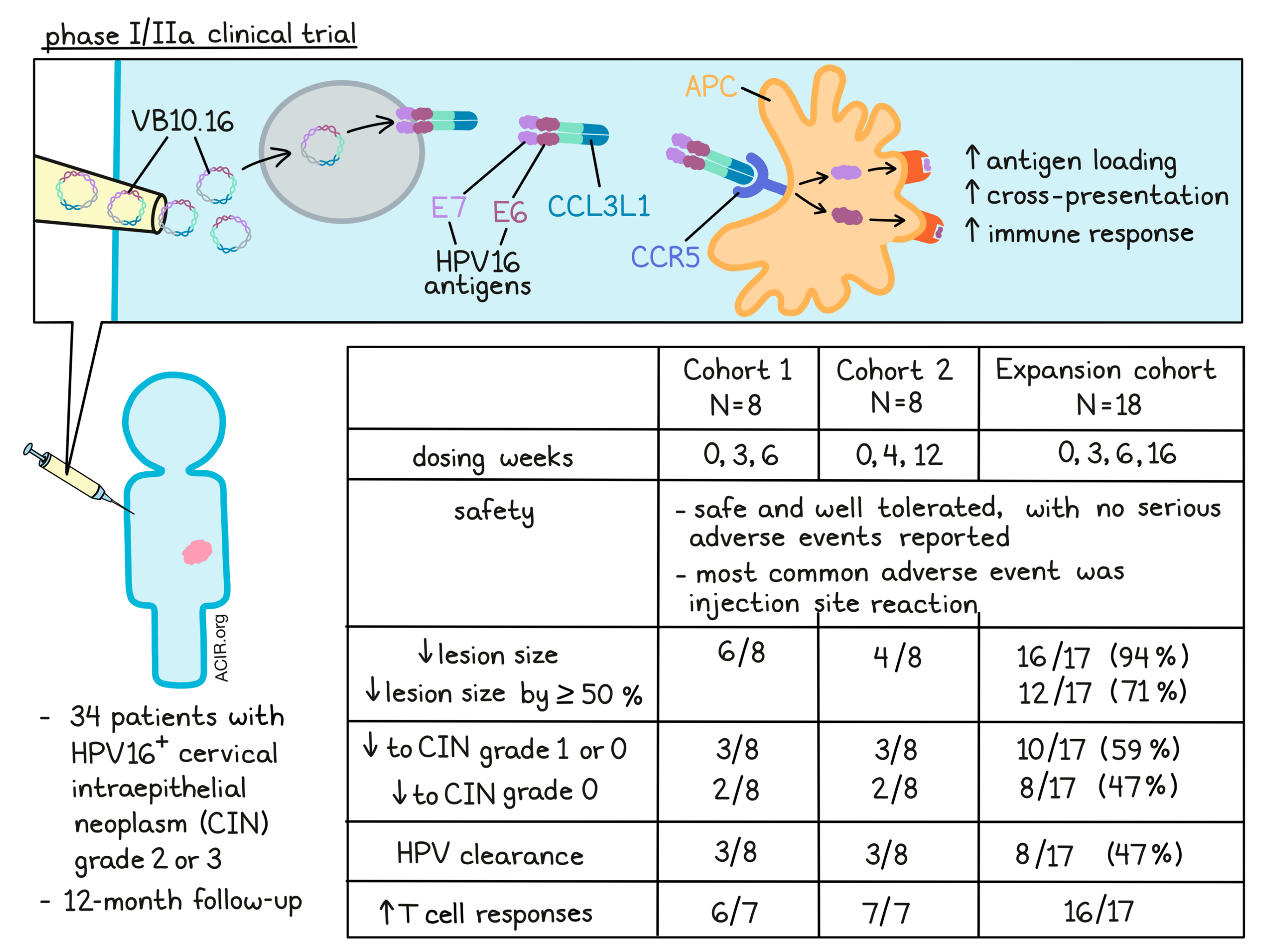
The purpose of this trial was to evaluate the clinical use of VB10.16, a therapeutic DNA-based vaccine in which the HPV16 antigens E6 and E7 are linked to CCL3L1. The inclusion of CCL3L1 targets CCR5 on antigen-presenting cells, enhancing antigen loading and cross-presentation via receptor internalization, and ultimately inducing a stronger immune response.
A total of 34 patients with HPV16+ CIN grade 2 or 3 were enrolled in the trial. In Cohort 1, 8 patients were vaccinated with 3mg VB10.16 at weeks 0, 3, and 6, while in Cohort 2, another 8 patients were vaccinated at weeks 0, 4, and 12. Later, based on the immunogenicity results from Cohorts 1 and 2, an Expansion cohort of 18 patients was vaccinated at weeks 0, 3, 6, and 16.
The primary endpoint of this trial was safety. Among the 34 treated patients, no serious adverse events (AEs) were reported, and no patients discontinued treatment due to AEs. All but one patient reported mild to moderate AEs, the most common of which was injection site reaction, which was mostly mild and resolved within a few days. 99% of all AEs were grade 1 or 2, though two patients reported grade 3 AEs, including headache, hyperesthesia, erythema, and injection site pain. No grade 4 or 5 AEs were reported. One patient also reported late-emerging AEs, including alopecia, influenza-like illness, and injection site pruritus. Overall, treatment was determined to be safe and well tolerated.
Moving on to their secondary endpoints, Hillemanns et al. assessed the preliminary efficacy of VB10.16 over a 12-month follow-up period. In the Expansion cohort (0, 3, 6, and 16 weeks dosing) , HPV16 clearance was seen in 8 (47%) of 17 of evaluable patients. Reduced lesion size was observed in 16 (94%) of 17 evaluable patients, with 12 (71%) patients showing lesion size reduction of 50% or more compared to baseline. 10 (59%) patients showed regression to grade 1 or 0 CIN, 8 (47%) of whom achieved complete regression to grade 0 CIN.
In the initial dosing cohorts, a reduction in lesion size was observed in 6 of 8 evaluable patients in Cohort 1 (0, 3, and 6 weeks dosing) and 4 of 8 evaluable patients in Cohort 2 (0, 4, and 12 weeks dosing). Regression of lesions to CIN grade 1 or 0 was observed in 3 patients in each cohort, complete regression to CIN grade 0 was observed in 2 patients in each cohort, and HPV clearance was observed in 3 patients in each cohort during 12 months of follow-up.
Looking more closely at the immune responses induced by VB10.16, the researchers measured systemic T cell responses by comparing IFNγ production by PBMCs in response to HPV16 E6 and E7 before and after vaccination. This showed that T cell responses were increased in 6 of 7 evaluable patients from cohort 1, and in all 7 evaluable patients from Cohort 2. Further, T cell responses increased with subsequent vaccinations and peaked after each boost, indicating the importance of a multi-dose vaccination regimen. Compared to Cohort 2, Cohort 1 showed faster, stronger, and longer-lasting immune responses. Together, these results informed the dosing regimen for the Expansion cohort, which mimicked the dosing regimen from cohort 1, but with an additional boost at week 16.
In the Expansion cohort, all 17 evaluable patients showed strong T cell responses, which were increased compared to baseline in 16 of the 17 patients. Further, the addition of the boost at week 16 amplified and prolonged immune responses compared to Cohort 1. Overall, 29 of 31 evaluable subjects showed vaccine-induced T cell responses against both E6 and E7 antigens, supporting the immunogenicity of VB10.16. Further, T cell responses correlated strongly with reduction in lesion size, and most patients with strong T cell responses and lesion size reduction presented with regression to CIN grade 1 or 0. These results suggest that VB10.16 induces a clinically relevant immune response.
Finally, the researchers looked at PD-L1 upregulation in CIN lesions following VB10.16 vaccination and identified a trend towards increased PD-L1 expression. Further, upregulation of PD-L1 (more than 1%) was observed in all 6 of the patients who failed to achieve a regression to CIN 1 or CIN 0, suggesting that induced PD-L1 upregulation may delay or hinder T cell-mediated elimination of target cells, and that combination with PD-1 axis blockade may be beneficial.
Overall, the results observed in this early clinical trial showed that VB10.16 was safe and well tolerated in patients with high-grade CIN. VB10.16 was also shown to induce strong immune responses, reduce grade and size of CIN lesions, and clear HPV16 in a high proportion of patients. These early results are promising and warrant further investigation in larger trials.
Write-up and image by Lauren Hitchings
Meet the researcher
This week, first author Peter Hillemanns answered our questions.

What was the most surprising finding of this study for you?
The Alpha carcinogenic HPV types, such as HPV16 and HPV18, have evolved superior immunoevasion strategies over hundreds of thousands of years, making immune therapy for HPV-associated cancers a big challenge. Therefore, it was great to see that our novel therapeutic HPV16 vaccine, which links antigens to a CCL3L1-targeting module, achieved a regression of lesion size and CIN grading in the majority of patients with cervical precancer. Furthermore, I was surprised to see that in our precancer cohort, the upregulation of PD-L1 was linked to the non-responder group. That could open the door for further immune therapeutic strategies.
What is the outlook?
Well, this upregulation provided a strong rationale for us to combine our vaccine VB10.16 with an anti-PD-1/PD-L1 checkpoint inhibitor. Certainly, this is not a suitable approach for cervical intraepithelial neoplasia, since its easy removal by loop electrosurgical excision procedure (conization) is highly effective. However, this stimulated us to initiate a phase 2 study of VB10.16 in combination with the PD-L1 inhibitor atezolizumab in women with HPV16-positive advanced cervical cancer (NCT04405349), which has already started.
What was the coolest thing you’ve learned (about) recently outside of work?
I love sports as a great balance to my intense clinical and academic life. I just started wing foiling which is great fun, but still quite challenging.



