In two recent papers published in Nature Medicine, researchers documented two mechanisms, one anticipated and one unexpected, for the relapse of B cell acute lymphoblastic leukemia (B-ALL) after CAR T cell treatment. Ruella, Xu, and Barrett et al. explored the unusual case of a 20-year-old male with B-ALL who enrolled in a clinical trial of CD19-directed CAR T cells. Following lymphodepletion, the patient was infused with CTL019 (a CD19-targeted autologous CAR T cell product), which successfully engrafted, expanded, tapered off, and persisted at low levels in the patient – as was expected. The patient achieved complete remission by day 28 and was routinely monitored long-term, until something unusual happened. At day 252 there was an unexpected second expansion of CAR19+ cells, but it did not align with expansion of CAR19+ T cells. At day 261 the patient experienced frank relapse, and immunophenotyping revealed that the observed CAR19 expression was coming from CAR-transduced leukemic B cells. Further therapies were attempted, including a CD22-directed CAR T cell therapy, however, the patient’s leukemic cells continued to expand and the patient ultimately died of complications due to the disease.
In an effort to understand the events leading to relapse and eventual death in this patient, Ruella, Xu, and Barrett et al. analyzed the cells of the relapsed disease and identified that CAR19+ leukemic cells at relapse had originated from a single leukemic B cell that had been inadvertently transduced with two copies of the CAR vector during the CAR T cell manufacturing process. In a retrospective analysis, the researchers found that the CAR19+ leukemia could be detected in the bone marrow three months prior to clinically evident relapse, and that CAR19+ B cell numbers progressively increased until disease became clinically evident.
The researchers next noted that by surface staining, the relapsed CAR19+ leukemic cells appeared to be CD19- and so they began to investigate the mechanism for the loss of CD19. They did not find evidence that insertional mutagenesis played a role, nor could they identify mutations in CD19, alternative splicing in CD19, or mutations in the B cell receptor complex protein CD81 in the patient. When the team analyzed mRNA and performed immunohistochemical analysis of the bone marrow with antibodies recognizing the intracellular domain CD19, they found that the CD19 protein was in fact being expressed, but that it could not be detected by flow cytometry or CD19-directed monoclonal antibodies.
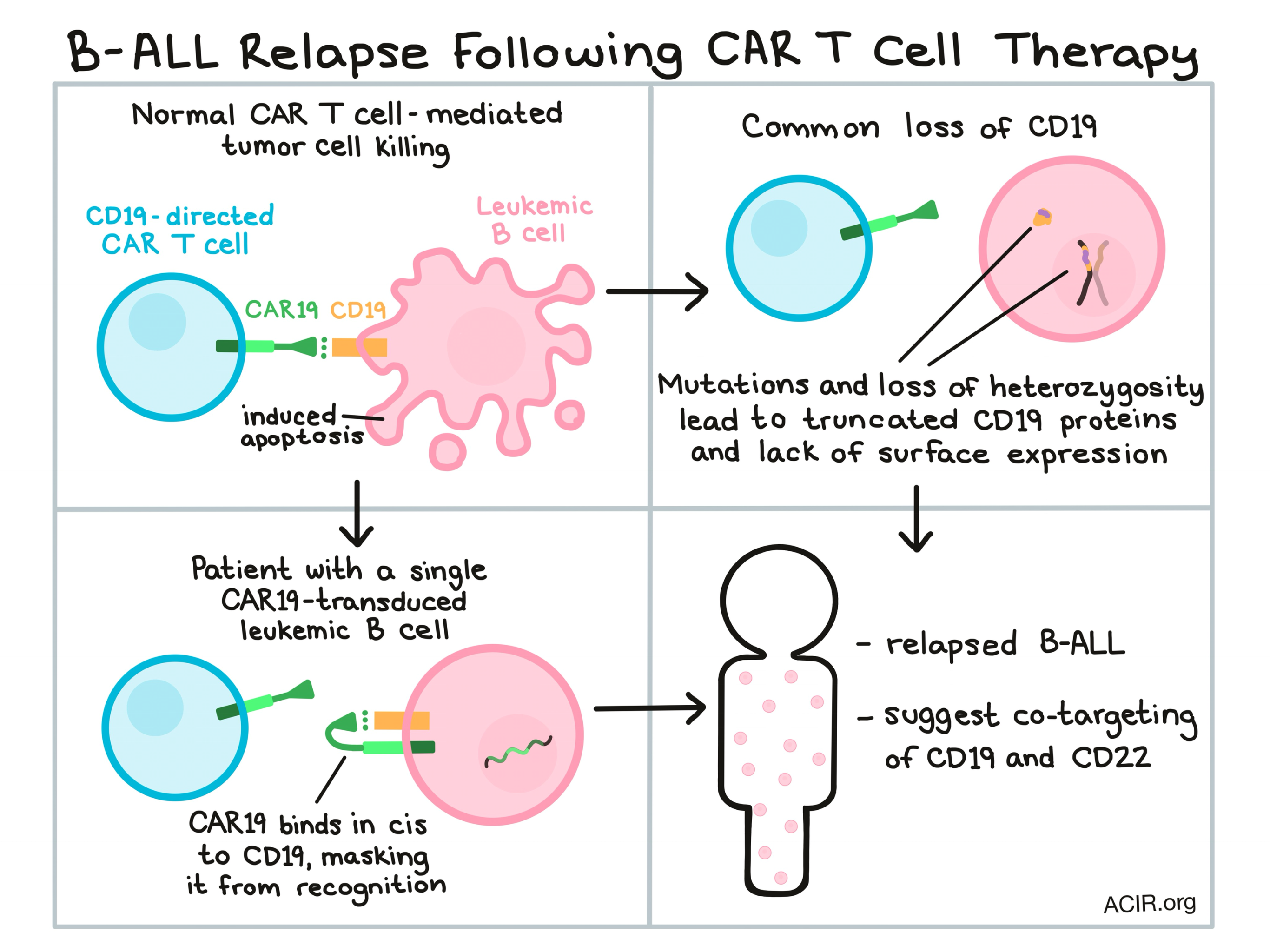
To determine whether CD19 was being expressed on the cell surface or intracellularly, Ruella, Xu, and Barrett et al. utilized confocal microscopy and found that CD19 was expressed on the cell surface, and moreover, that it colocalized with CAR19. The researchers hypothesized that the CAR19 and CD19 were binding in cis, masking the CD19 from detection and conferring resistance to CD19-targeted CAR T cells. This “epitope masking” hypothesis was confirmed when the researchers recreated the phenomenon on a B-ALL cell line transduced with CAR19, causing what appeared by flow cytometry to be a dramatic loss of CD19 expression. Further, the team was able to recreate the same effect using CD22+ cells and CD22-targeted CAR.
While CAR19+ leukemia-driven relapse was only observed in this one case, the researchers evaluated the extent to which other patients might be at risk. They found that the frequency of leukemic B cells in samples at the time of apheresis (before CAR T cell manufacturing) correlated with the frequency of leukemic B cells that end up in the final CAR T cell product. The patient in this case study had one of the highest initial CD19+ contents, although several other patients with higher leukemic content did not develop the same problem. One other relapsed patient was found to have CAR19+ leukemia cells, but they accounted for only a minor subset of relapsing cells and were unlikely the drivers of relapse in this patient.
While the transduction of leukemic cells with CARs and the subsequent masking of CD19 was a rare incident, it is fairly common for tumors to lose CD19 expression to escape recognition during CAR19 T cell therapy. Orlando et al. evaluated the genetic mechanisms by which tumors lose targeted antigens to evade elimination under the pressure of CAR T cell therapy. The researchers in this study analyzed specimens from initial disease screening and relapsed disease and found that 12 of the 17 relapsed patients they evaluated had CD19- leukemia. In all 12 cases of CD19- relapse, the researchers identified mutations throughout exons 2-5 of the CD19-encoding gene, with each patient showing at least one frameshift mutation. Mutations in these exons would lead to a truncated protein lacking membrane anchorage, resulting in the loss of function of CD19.
Interestingly, in cases of CD19- relapse, leukemic B cell populations were entirely or almost entirely CD19-, suggesting that mutations in CD19 were either biallelic or that secondary alleles were in some way silenced. In 8 of 9 evaluable relapsed patients, the researchers identified an acquired loss of heterozygosity. Some previous research had pointed to alternative splicing or lineage switching as a cause of loss of CD19 function, but neither was observed in this data set.
To better understand the timeline along which patients move from complete remission to relapse, Orlando et al. sequenced samples from various time points. They found that the genetic variants observed at relapse were not detectable before relapse, even in samples taken as shortly as 1 month before relapse, indicating that relapse closely follows the emergence of CD19 loss-of-function mutations.
Whether CD19 is masked (as in the single case studied by Ruella, Xu, and Barrett et al.) or lost (as in the several patients studied by Orlando et al.), the ability of tumors to hide from CD19-targeted CAR T cell therapy represents a major threat to treated patients. Both Ruella, Xu, and Barrett et al. and Orlando et al. suggest the possibility of targeting additional B cell antigens, such as CD22, to reduce the likelihood of tumor escape. The potential of CAR T cell therapies is still great, but understanding how and why CAR T cell therapy fails in some patients is essential in improving patient outcomes and expanding the number of patients who durably benefit.
by Lauren Hitchings



