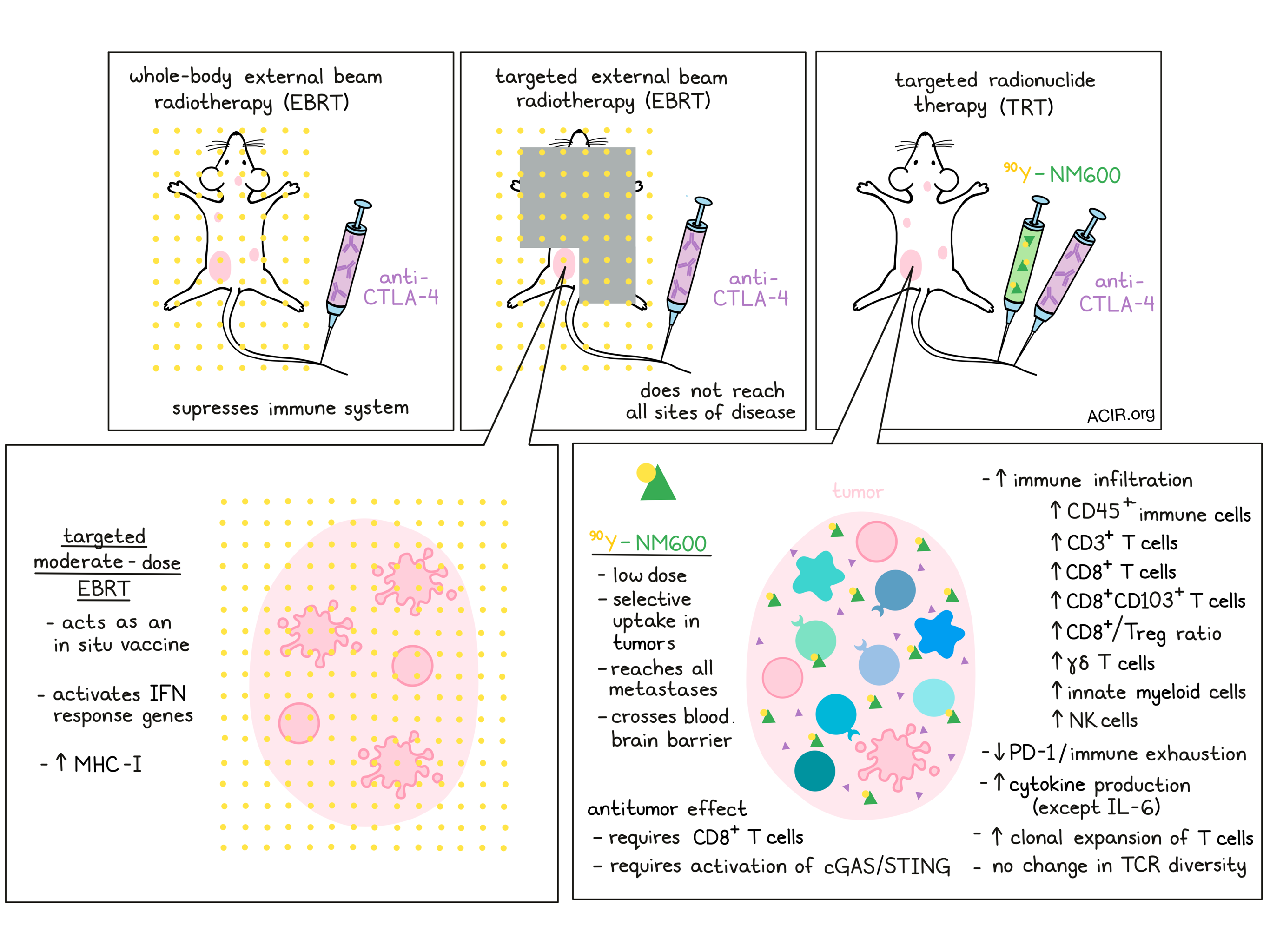
In the setting of cancer, radiotherapy can directly damage or kill tumor cells, and can act as an in situ vaccine that triggers antitumor immunity; the contribution of each of these mechanisms varies based on the dose. In most cases, radiation is delivered as targeted external beam radiotherapy (EBRT), but not all tumors and metastases are accessible for treatment. Patel et al. recently investigated the possibility of delivering low-dose radiotherapy through targeted radionuclide therapy (TRT). This strategy utilized an alkylphosphocholine analog, NM600, which is robustly taken up by a variety of mammalian tumors, to carry and deliver radioactive yttrium (90Y). 90Y-NM600 was tested in a variety of models and in combination with a variety of therapies. The results were recently published in Science Translational Medicine.
Patel et al. began by using PET imaging, pharmacokinetic biodistribution studies, and dosimetry calculations to show that 90Y-NM600, delivered intravenously into mice bearing B78 (a B16 melanoma derivative), NXS2, or 4T1 flank tumors, preferentially accumulates in tumors, especially in larger tumors, compared to in normal tissue. Using a dose that was previously shown to not reduce white blood cell or lymphocyte counts, the researchers showed 90Y-NM600 could also be safely combined with anti-CTLA-4 without significant toxicity.
Next, the researchers evaluated the potential antitumor efficacy of 90Y-NM600 in various settings. In combination with anti-CTLA-4, 90Y-NM600 improved antitumor responses and increased survival in a dose-dependent manner. The two highest doses of 90Y-NM600, 50 μCi and 100 μCi, enhanced the efficacy of CTLA-4 to a similar degree, so 50 μCi was used going forward. In addition to the dose, the researchers evaluated the effects of the timing and sequence of the dose, and found that the variations tested had little impact on the success of therapy. The addition of anti-PD-1 to this regimen also did little to improve the effects. Only mice that received 90Y-NM600 in combination with immunotherapy achieved complete responses, and responding mice rejected rechallenge with the same tumor after 90 days. Further, mice bearing 4T1 tumors, which spontaneously develop metastases, showed reduced numbers of metastatic lung nodules when treated with 90Y-NM600 and anti-CTLA-4.
A major potential advantage TRT compared to EBRT is the ability to reach and treat all sites of metastatic disease without suppressing the immune system. Comparing these different treatment strategies, Patel et al. treated tumor-bearing mice with anti-CTLA-4 plus targeted EBRT, whole-body EBRT, or TRT. Mice treated with targeted EBRT or TRT showed similar antitumor responses, but the effect was lost in mice treated with systemic EBRT, likely due to systemic immunosuppression. Consistent with this, the antitumor effects of EBRT and TRT were dependent on T cells.
Evaluating the mechanism behind the antitumor effect of TRT versus low- and moderate-dose EBRT, Patel et al. looked at the tumor immune environments in treated mice. Moderate-dose EBRT initially decreased infiltrating immune cells, but these cells rebounded at days 7 at 14. Low-dose TRT on the other hand, improved the tumor immune environment starting at day 1, with increased innate myeloid cells and natural killer cells, and an increased CD8+ T cell/Treg ratio. Looking at immune-related gene expression, the researchers also observed a number of changes that began at day 1, peaked at day 7, and were trending towards baseline by day 14. These included a modest decrease in Il6 in TRT-treated mice, an increase in Vcam1 in TRT- and low-dose EBRT-treated groups, and increased expression of Fas (indicative of apoptosis) across treatment groups. Increased IFNβ, indicative of increased activation of the cGAS/STING pathway, was also observed across all groups, though the moderate-dose EBRT group showed the greatest increases in downstream type I IFN response genes and MHC-1. Still, activation of the cGAS/STING pathway was found to be required for antitumor efficacy in TRT-treated mice as well.
Further investigating changes in the TME induced by TRT plus anti-CTLA-4, the researchers observed increased CD45+ immune cells, CD3+ T cells, CD8+ effector T cells, CD8+CD103+ tissue resident effector memory T cells, and γδ T cells. They also saw a decrease in PD-1, suggesting reduced immune exhaustion. Most cytokines also increased in the TME, particularly in responding mice. One exception was IL-10, which was reduced in the TME, consistent with a reduction of infiltrating Tregs or suppressive monocyte populations. Ex vivo, TILs isolated from combination-treated animals produced more IFNγ upon stimulation. Further, an increase in clonal expansion of T cells was also observed through deep TCRβ sequencing. Interestingly, an increase in T cell diversity was not observed, despite the fact that EBRT and immune checkpoint therapy treatment had previously been shown to increase T cell diversity.
Given that targeted moderate-dose EBRT and low-dose TRT have distinct mechanisms for eliciting antitumor efficacy, Patel et al. hypothesized that they could be combined for an additive effect. Delivered together, these two forms of radiotherapy enhanced the antitumor effect of CTLA-4 more than either individual treatment, and a strong abscopal effect was observed. Mice that experienced a complete response in both tumors (B78) were resistant to rechallenge with the same tumor line, and most were resistant to a later rechallenge with the parental B16 melanoma, which shares common antigens.
To test the safety and feasibility of 90Y-NM600 in a larger animal model that would more closely mimic human patients, Patel et al. turned to companion canines with cancer. Two dogs with metastatic cancer (osteosarcoma and melanoma) were enrolled in the study and were treated with a combination of targeted EBRT and systemic TRT. Imaging showed semi-selective uptake of 90Y-NM600 into the primary tumors and in all documented metastasis. Little evidence of toxicity was observed through laboratory testing, and no adverse events occurred. Uptake of 90Y-NM600 was also low enough in the bone marrow that the systemic radiation did not induce immunosuppression from bone marrow depletion.
Overall, Patel et al. showed that TRT, delivered in the form of 90Y-NM600, can safely modulate tumor immune environments and enhance the effectiveness of immune checkpoint blockade. Because 90Y-NM600 is selectively taken up by tumors, it can be delivered systemically and can reach tumor metastases that may not be accessible for treatment with radiotherapy through EBRT. Further, as these two forms of radiotherapy work through different mechanisms, they could be combined to further enhance the efficacy of immune checkpoint blockade, particularly with anti-CTLA-4.
Write-up and image by Lauren Hitchings
MEET THE RESEARCHER
This week, first author Ravi Patel answered our 3 questions.
What prompted you to tackle this research question?
As a radiation oncologist, I’ve always felt that we were limited in our ability to treat patients with metastatic cancer. At most, we could only offer disease palliation for these patients. When I was completing residency, I wanted to work on research in which I could make a meaningful impact in treating these patients’ disease with novel radiation approaches. Therefore, I decided to pursue a Benston Research Fellowship with Dr. Zach Morris and Dr. Paul Sondel to study combination radiation immunotherapy approaches. I was fortunate enough to fall into an early collaboration between the Morris-Sondel group and Dr. Jamey Weichert, where they were working on using targeted radiotherapy in combination with an immunocytokine (anti-GD2-IL2) developed by their group. For my project, I chose to work on a bit broader approach, testing the ability of these targeted radiotherapy agents to enhance the efficacy of standard clinical immune checkpoint inhibitors in a tumor agnostic fashion. I’m excited about our initial results and I believe this type of systemic low-dose targeted radiotherapy approach can make an impact in improving outcomes in patients with metastatic cancer.
What was the most surprising finding of this study for you?
The most surprising finding from our study was that such low doses of radiation were able to stimulate such a strong antitumor immune response when combined with checkpoint blockade in these immunotherapy-resistant tumor models. For example, studies in hepatocellular carcinoma have shown that radiation doses ranging from 120 to more than 200 Gy are needed to treat with Yttrium-90 monotherapy in these relative radiosensitive tumors. In contrast, our study utilizes Yttrium-90 radiation absorbed in doses of approximately 2.5 Gy to enhance the efficacy of immune checkpoint blockade. Moreover, we found that additional targeted radiopharmaceutical therapy dose escalation didn’t lead to further gains in efficacy. This finding was a surprise to us; however, it can help us greatly limit toxicity in patients when we translate this approach into human trials.
What was the coolest thing you’ve learned (about) recently outside of work?
I’m in Pittsburgh now and loving my new city, but since I started this project in Wisconsin, I’ll mention a hobby I picked up there. As many people know, Wisconsin has many wonderful lakes, so during my research fellowship I decided to join a sailing club. I learned to sail at the same time as I started this research project and learned about cancer immunotherapy (both areas were completely new to me at the time). As a new sailor, I often found myself initially struggling, since my instinct was to fight the wind and I would find myself “In Irons” or too “close-hauled” for the conditions. However, as I gained experience, I learned to let the wind guide me and make more subtle adjustments. Looking back, the lessons I learned sailing were also applicable to my research work, as well as outside life.




