The tumor immune microenvironment (TIME) of ER+HER2- high-risk early breast cancer is generally immune-cold, which limits immune checkpoint blockade (ICB) responses. Since radiotherapy may modulate the immune response, it may increase ICB efficacy. However, radiotherapy may also activate the immunosuppressive CD73-adenosine pathway. Based on these hypotheses, De Caluwé et al. conducted a clinical trial assessing the use of neoadjuvant chemotherapy (NACT) and immune-modulating stereotactic body radiation therapy (iSBRT), alone or in combination with anti-PD-L1 and anti-CD73. Efficacy, safety, and biomarker data were recently published in Nature Medicine.
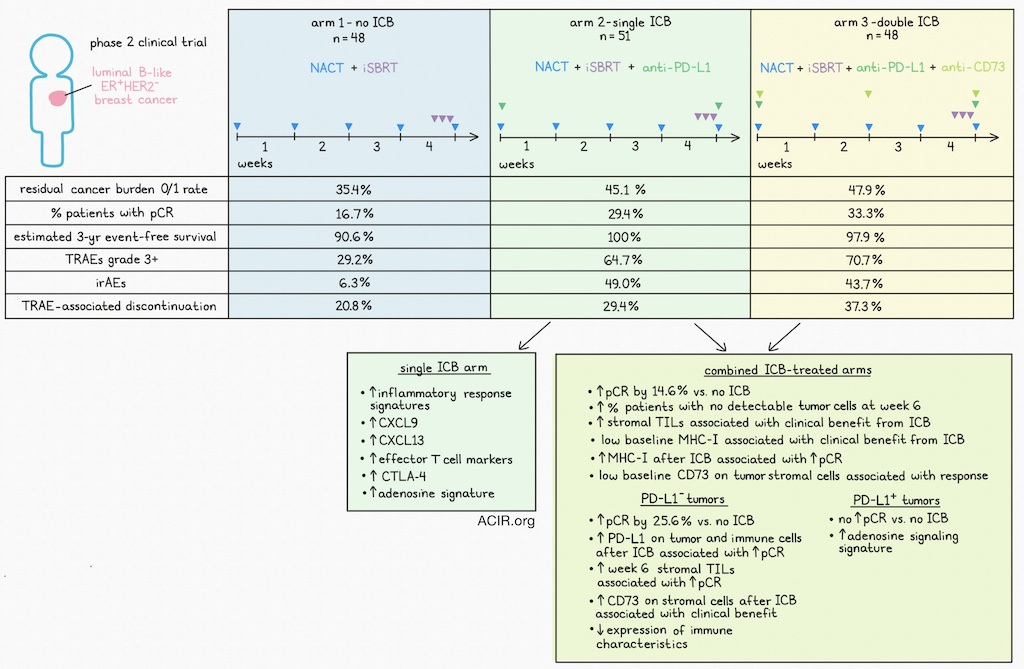
The Neo-CheckRay trial was a phase 2, randomized, multicenter trial for patients with luminal B-like (MammaPrint High-Risk) ER+HER2- breast cancer. The trial had three arms: NACT and iSBRT alone (No ICB group; n=48); NACT, iSBRT, and the anti-PD-L1 antibody durvalumab (Single ICB; n=51); or NACT, iSBRT, anti-PD-L1, and the anti-CD73 antibody oleclumab (Double ICB; n=48). NACT and ICB treatment was initiated on day 1, with NACT provided for 19 weeks and ICB for 17 weeks at varying intervals. iSBRT (24 Gy delivered as three fractionated doses on continuous days) was initiated at the end of week 4.
The primary endpoint of this trial was the residual cancer burden (RCB) 0/1 rate, and the secondary endpoint was the pathologic complete response (pCR) rate, evaluated at the time of surgery. The RCB 0/1 rate was 35.4% in the No ICB arm, 45.1% in the Single ICB arm, and 47.9% in the Double ICB arm. The percentages of patients achieving a pCR were 16.7% in the No ICB group, 29.4% in the Single ICB group, and 33.3% in the Double ICB group.
PD-L1 expression was evaluated as the percentage of tumor area covered with PD-L1-expressing immune cells. Among patients with PD-L1-negative (<1%) tumors, those treated in the ICB arms experienced significantly higher pCR rates compared to those in the No ICB arm. In the PD-L1-positive group (≥1%), however, no differences in pCR rates were observed among the three arms. A significant benefit from ICB (Single or Double) was observed in node-positive patients with PD-L1-negative tumors.
After a median follow-up of 34 months, the estimated 3-year event-free survival rate was 90.6% for No ICB, 100% for Single ICB, and 97.9% for Double ICB. There were no deaths in this trial.
Treatment-related adverse events (TRAEs) of grade ≥3 were observed in 29.2% of patients in the No ICB (serious TRAE: 8.3%), 64.7% in the Single ICB (serious TRAE: 21.6%), and 70.7% in the Double ICB (serious TRAE: 20.9%) groups. Study treatment was discontinued due to TRAEs in 20.8%, 29.4%, and 37.3% of cases in the No ICB, Single ICB, and Double ICB arms, respectively. Immune-mediated AEs were observed in 6.3% of the No ICB group, 49.0% of the Single ICB group, and 43.7% of the Double ICB group.
When the researchers grouped the two ICB arms and compared them with the No ICB arm, the addition of ICB led to a significant 14.6% increase in pCR among all patients, rising to a 25.6% increase in the PD-L1-negative subgroup.
To determine whether baseline tumor characteristics correlated with treatment response, the researchers analyzed various biomarkers. Patients with Ultra-High MammaPrint or a higher Ki67 index had higher pCR rates, but no benefit of adding ICB was observed compared to patients with MammaPrint High-Risk index. No patients with MammaPrint Low-Risk disease achieved a pCR.
Assessing the TIME showed that PD-L1-negativity and the presence of stromal TILs were associated with greater benefit from the addition of ICB. The baseline median stromal TIL percentage was 10% in patients who achieved pCR, and 1% in those without pCR.
On-treatment biopsies obtained at week 6 (~1 week after iSBRT) were assessed for tumoral and immune PD-L1 expression. A subset of PD-L1-negative tumors became PD-L1-positive at week 6, with the increase of expression mainly observed on immune cells, and this most commonly occurred in the ICB arms. An increase in PD-L1 expression on immune and tumor cells was associated with a high pCR rate in the ICB arms, but only in patients whose tumors were PD-L1-negative at baseline.
A higher percentage of patients in the ICB arms had no detectable tumor cells at week 6 than in the no ICB arm, which was associated with higher pCR rates. No significant increases in stromal TIL levels were detected after treatment, and the percentage of patients with stromal TIL-positive tumors decreased in all treatment arms. However, in PD-L1-negative tumors treated with ICB, an increase in stromal TILs at week 6 was associated with pCR benefit.
The researchers then investigated immune escape mechanisms modulated by iSBRT. Patients with low MHC-I expression at baseline benefited most from the addition of ICB to iSBRT, and an increase in MHC-I expression in tumor and stroma significantly correlated with pCR in patients receiving ICB. The researchers hypothesized that iSBRT may upregulate CD73. CD73 expression was primarily observed in the stroma, and lower baseline stromal CD73 levels correlated with a better response to iSBRT and ICB. At week 6, stromal CD73 decreased in all treatment groups, but this was not associated with improved pCR, while an increase in stromal CD73 was associated with benefit from the addition of ICB in the PD-L1-negative population.
Finally, bulk RNAseq was performed on paired baseline and week 6 samples to evaluate immune-related pathways. At baseline, PD-L1-negative tumors had lower expression of many immune-related characteristics. In PD-L1-positive tumors, the adenosine signaling signature was significantly upregulated compared with PD-L1-negative tumors.
In 75 paired biopsies that still had tumor cells present at week 6, the Single ICB arm showed increased expression of inflammatory response signatures, CXCL9, CXCL13, effector T cell markers, CTLA-4, and the adenosine signature. The other two arms had lower immune activation. The treatment-induced immune activation at week 6 was primarily observed in PD-L1-negative tumors in the Single ICB arm.
Together, the results from this trial show the immunomodulating effects of iSBRT with NACT, anti-PD-L1, and anti-CD73 in patients with high-risk ER+HER2- early breast cancer. The data on PD-L1, MHC-I, and adenosine pathway changes in response to therapy suggest that the main benefit from this treatment strategy is among patients with immune-cold tumors. Further validation of these biomarker data could support their use in selecting patients who might benefit most from this treatment strategy.
Write-up by Maartje Wouters, image by Lauren Hitchings
Meet the researcher
This week, first author Alex de Caluwé answered our questions.
What was the most surprising finding of this study for you?
We were excited to find that delivering 3 × 8 Gy to the primary breast tumor appeared to overcome resistance to anti-PD-L1 immune checkpoint inhibition in patients with baseline PD-L1-negative tumors. Early on-treatment biopsies at week 6 suggested that radiation therapy reprogrammed the tumor microenvironment toward a more inflamed phenotype. Although this was our central hypothesis, we were surprised by the magnitude of the effect in the PD-L1-negative subgroup. Another unexpected finding was that many patients already had no residual tumor on the week 6 biopsy, which strongly correlated with pathological complete response nearly 19 weeks later at surgery. Perhaps the most intriguing observation was that even low-dose radiation (around 1 Gy) to the axillary lymph nodes appeared to diminish the benefit of immunotherapy, in line with emerging preclinical evidence highlighting the importance of preserving tumor-draining lymph nodes.
What is the outlook?
The next step is to validate these findings in a larger phase III trial powered for event-free survival. Beyond ER-positive/HER2-negative breast cancer, we believe this strategy has the potential to be translated to other breast cancer subtypes and, more broadly, to immunologically "cold" cancers, where immune checkpoint inhibitors have shown limited activity. If confirmed, this approach could provide a simple and widely accessible way to enhance the efficacy of cancer immunotherapy.
Who or what has been a major source of inspiration or motivation for you throughout your career?
Martine Piccart and Laurence Buisseret have been major sources of inspiration throughout my career. They are visionary medical oncologists who consistently look beyond the boundaries of their own specialty to identify new research opportunities. This trial is a perfect example of how meaningful advances in cancer treatment arise from true multidisciplinary collaboration, bringing together radiation oncologists, medical oncologists, pathologists, translational scientists, and many others to shape the future of oncology together.



